Synopsis
Compound overview
- Research only
- In clinical trials
- Approved outside US
- FDA-approved
What it is
Enclomiphene is one of the two isomers that make up clomiphene. It was developed on its own as a potential treatment for low testosterone in men and completed late-stage trials, but it did not gain FDA approval.
What it does
How it has been studied:
- Studied as a treatment for low testosterone in men
- Designed to raise testosterone while preserving fertility
- Completed late-stage clinical trials
- Did not receive FDA approval
How it works
Enclomiphene blocks estrogen receptors in the brain, prompting the release of LH and FSH, which in turn signal the testes to make more testosterone — without shutting down sperm production the way testosterone injections can.
Safety notes
Despite completing trials, enclomiphene is not an FDA-approved drug, so it is sold without that oversight. Reported effects include headache and mood changes, and as a SERM it shares clomiphene's risk profile. Material sold by research vendors is unregulated and not pharmacy-grade.
Where to buy Enclomiphene Citrate
Standard lyophilized vial — reconstitute and measure doses yourself. The conventional research format.
Affiliate links — we may earn a commission at no extra cost to you.
Molecular Structure
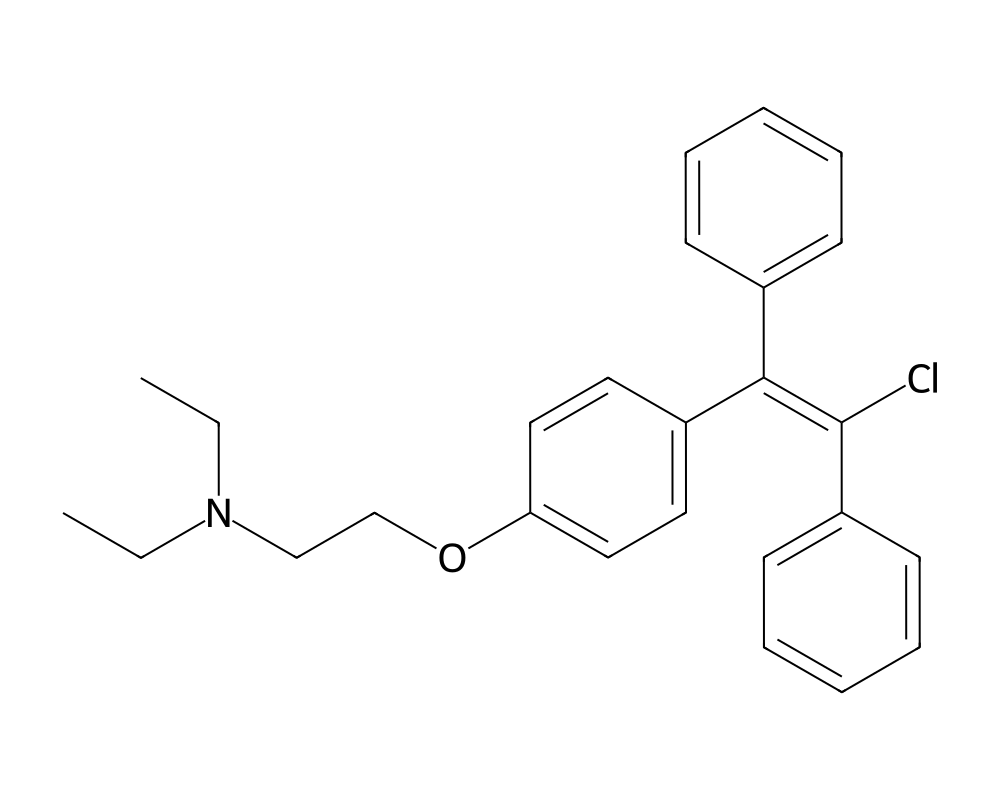
Overview
Enclomiphene citrate is the trans-isomer of clomiphene citrate, a selective estrogen receptor modulator (SERM) that has been used in fertility medicine for decades. While the racemic mixture of clomiphene contains both the zuclomiphene (cis) and enclomiphene (trans) isomers, pharmaceutical researchers isolated enclomiphene because it carries the bulk of the estrogenic antagonist activity without the prolonged estrogenic agonist effects attributed to zuclomiphene. The compound was developed by Repros Therapeutics under the brand name Androxal, targeting secondary hypogonadism in men who retain functional testes but suffer from insufficient gonadotropin signaling.
Contents
The rationale behind isolating the trans-isomer is straightforward. Zuclomiphene has a half-life measured in weeks and tends to accumulate with repeated dosing, producing unwanted estrogenic stimulation. Enclomiphene clears the body within days, offering a cleaner pharmacological profile. For researchers studying hypothalamic-pituitary-gonadal (HPG) axis restoration, this distinction matters enormously. The compound represents a more targeted tool for investigating how estrogen receptor blockade at the hypothalamus can restore endogenous testosterone production.
Mechanism of Action
Enclomiphene works by competitively binding to estrogen receptors in the hypothalamus and pituitary gland. Under normal physiological conditions, circulating estradiol provides negative feedback to the hypothalamus, suppressing the release of gonadotropin-releasing hormone (GnRH). When enclomiphene occupies these receptors, the hypothalamus interprets the situation as a low-estrogen environment, regardless of actual circulating estradiol levels.
This triggers an increase in GnRH pulse frequency, which in turn stimulates the anterior pituitary to release more luteinizing hormone (LH) and follicle-stimulating hormone (FSH). LH acts on Leydig cells in the testes to increase testosterone synthesis, while FSH supports spermatogenesis by acting on Sertoli cells. The net result is elevated endogenous testosterone and preserved or improved fertility, a critical distinction from exogenous testosterone replacement, which suppresses both LH and FSH and typically impairs sperm production.
Unlike aromatase inhibitors, which reduce estrogen synthesis directly, enclomiphene leaves circulating estradiol levels largely intact. It simply prevents that estradiol from exerting its negative feedback effects. This preserves the physiological roles of estrogen in bone metabolism, cardiovascular function, and lipid regulation while still disinhibiting the HPG axis.
Research Summary
Clinical trials conducted by Repros Therapeutics demonstrated that enclomiphene citrate could reliably increase serum testosterone levels in men with secondary hypogonadism. In the phase III ZA-301 and ZA-302 studies, subjects receiving 12.5 mg and 25 mg daily doses showed statistically significant increases in total testosterone compared to placebo, with many reaching the eugonadal range within weeks of initiation.
A notable finding across multiple studies was the preservation of sperm parameters. While topical testosterone gels and injections consistently suppress spermatogenesis, often to azoospermic levels, enclomiphene-treated subjects maintained or improved sperm counts. This finding positioned the drug as a potential alternative for hypogonadal men who wished to preserve fertility.
Research has also examined enclomiphene in the context of post-cycle therapy (PCT) following anabolic steroid use. Preclinical and observational data suggest the compound can accelerate recovery of endogenous testosterone production after HPG axis suppression, though controlled trials in this specific population remain limited. Studies on body composition have shown modest improvements in lean mass and reductions in fat mass, consistent with the testosterone-elevating effects.
The FDA declined to approve Androxal in 2015, citing manufacturing and quality control concerns rather than efficacy or safety failures. This regulatory setback did not diminish scientific interest; rather, it redirected research toward understanding the compound’s pharmacokinetics and long-term effects in greater detail.
Dosing in Published Research
About this section
The information below reports dosing only as it appears in published clinical or preclinical research and official regulatory documents. It is provided as published-literature reference material. It is not dosing guidance, not medical advice, and not a recommendation to use or self-administer this compound.
Enclomiphene citrate is the trans-isomer of clomiphene. It has been investigated as a treatment for secondary hypogonadism in men but is not FDA-approved, so it has no labeled dose. In a published Phase 2 study in men with secondary hypogonadism, three oral doses were compared: 6.25 mg, 12.5 mg and 25 mg taken once daily over six weeks, with the 25 mg dose producing the largest rise in testosterone. These figures describe what was administered in that specific trial.
Research doses, not a protocol
These doses come from a short clinical study of an investigational compound, not an established or recommended regimen. Enclomiphene is not FDA-approved, and material sold for research use is not a regulated drug product.
Safety and Side Effects
The safety profile of enclomiphene in clinical trials was generally favorable. The most commonly reported adverse effects included headache, nausea, and hot flashes, all consistent with SERM class effects. Visual disturbances, a known concern with racemic clomiphene, were reported less frequently with the isolated trans-isomer, supporting the hypothesis that zuclomiphene contributes disproportionately to ocular side effects.
Elevations in LH and FSH beyond physiological ranges were observed at higher doses, raising theoretical concerns about overstimulation of gonadal tissue. However, no clinically significant adverse events related to this overstimulation were reported in the published trial data. Liver function parameters remained stable across study durations of up to six months.
Long-term safety data beyond 12 months remain sparse. Researchers have flagged the need for studies examining bone mineral density, cardiovascular markers, and prostate health over extended treatment periods. The theoretical risk of estrogen receptor modulation affecting breast tissue or endometrial tissue (in potential off-label female use) also warrants continued investigation.
Current Research Status
Enclomiphene citrate remains an investigational compound. It has not received FDA approval for any indication, though it continues to be studied in academic and clinical settings. Research interest has grown substantially in the context of male hypogonadism management, where clinicians seek alternatives to testosterone replacement that do not compromise fertility. Several ongoing studies are investigating optimal dosing regimens, long-term safety profiles, and potential applications in metabolic syndrome and obesity-related hypogonadism. The compound is available through research chemical suppliers and select compounding pharmacies, though its regulatory status varies by jurisdiction.
Further reading: Enclomiphene: The SERM Studied for Testosterone reviews the clinical research on this selective estrogen receptor modulator.
Frequently Asked Questions
What is enclomiphene citrate?
Enclomiphene is the trans-isomer of clomiphene, a selective estrogen receptor modulator (SERM). It was developed on its own as a potential treatment for low testosterone in men and completed late-stage trials, but it did not gain FDA approval.
How does enclomiphene work?
Enclomiphene competitively blocks estrogen receptors in the hypothalamus and pituitary. This removes estrogen’s negative feedback, prompting increased release of gonadotropins, which in turn stimulate the testes to produce more testosterone.
Is enclomiphene FDA-approved?
No. Enclomiphene remains an investigational compound and has not received FDA approval for any indication, although it continues to be studied, particularly for male hypogonadism.
What does the research say about enclomiphene?
Phase III trials by Repros Therapeutics (the ZA-301 and ZA-302 studies) showed that daily enclomiphene at 12.5 mg and 25 mg significantly raised serum testosterone in men with secondary hypogonadism while aiming to preserve fertility.
What are the safety concerns with enclomiphene?
In clinical trials the safety profile was generally favorable. The most commonly reported adverse effects were headache, nausea and hot flashes, consistent with SERM class effects. Visual disturbances, a known concern with racemic clomiphene, were reported less frequently.
Research Handling & Storage
Storage
- Unopened: Store at controlled room temperature, 20–25°C (68–77°F), away from direct sunlight, heat, and moisture.
- Opened: Keep container tightly closed. Use within the timeframe indicated on the label, typically 30–90 days after opening.
- Do not freeze liquid solutions unless specifically indicated.
Handling Precautions
- Handle with appropriate personal protective equipment (PPE) including nitrile gloves, lab coat, and eye protection.
- Use aseptic/sterile technique when reconstituting and transferring solutions to prevent contamination.
- Avoid repeated freeze-thaw cycles which may denature the compound and reduce potency.
- Keep detailed laboratory records including reconstitution dates, lot numbers, concentrations, and storage conditions.
- Dispose of unused material and sharps in accordance with local regulations and institutional biosafety guidelines.
Stability & Shelf Life
Liquid formulations typically remain stable for 1–2 years when stored at the recommended temperature in the original sealed container. Once opened, potency may gradually decrease. Monitor for any changes in color, clarity, or odor, which may indicate degradation.
Purity & Quality Considerations
Research-grade compounds should be accompanied by a Certificate of Analysis (COA) confirming purity, typically verified by High-Performance Liquid Chromatography (HPLC) and Mass Spectrometry (MS). Look for purity levels of ≥98% for research applications. Third-party testing adds an additional layer of quality assurance. Always verify the source and documentation before using any research compound.
Research Supplies & Resources
Essential supplies and educational resources for peptide research. Links go to Amazon.com.
Lab Supplies
Recommended Reading
Lab Equipment
As an Amazon Associate, peptides.fyi earns from qualifying purchases. Learn more.