Synopsis
Compound overview
- Research only
- In clinical trials
- Approved outside US
- FDA-approved
What it is
Triptorelin is a synthetic analogue of GnRH, the hormone that controls the body's sex-hormone system. It is an FDA-approved prescription medicine (sold as Trelstar and other brands), used mainly to treat advanced prostate cancer and certain other hormone-related conditions.
What it does
Documented clinical uses include:
- Used to treat advanced prostate cancer
- Lowers testosterone or estrogen as part of treatment
- Used for endometriosis and early puberty in some cases
- Has documented clinical data
How it works
Triptorelin first stimulates, then with continued use suppresses, the pituitary's release of the hormones that drive testosterone and estrogen production — effectively lowering sex-hormone levels.
Safety notes
Triptorelin is a prescription cancer and hormone medicine used under specialist supervision. Side effects include hot flushes, bone-density loss and an initial hormone "flare". It is not a casual research compound, and research-vendor material is not pharmacy-grade.
Where to buy Triptorelin
Standard lyophilized vial — reconstitute and measure doses yourself. The conventional research format.
Affiliate links — we may earn a commission at no extra cost to you.
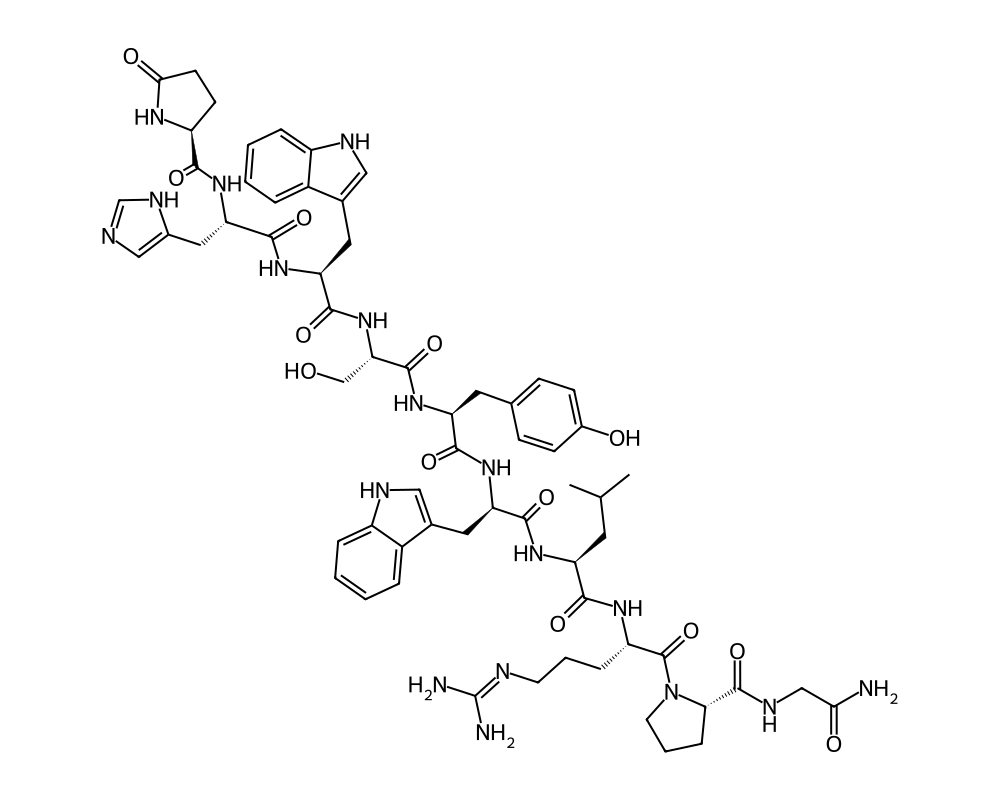
Molecular Structure
Research tool
Reconstitution calculator
Concentration
2.50mg/mL
Draw volume
0.10mL
Insulin units
10IU
Doses/vial
20
Overview
Triptorelin is a synthetic decapeptide analog of gonadotropin-releasing hormone (GnRH), also known as luteinizing hormone-releasing hormone (LHRH). It is one of several GnRH agonists developed for clinical use, alongside compounds such as leuprolide, goserelin, and buserelin. What distinguishes triptorelin from natural GnRH is a single amino acid substitution at position 6 (D-tryptophan replaces glycine), which dramatically increases its resistance to enzymatic degradation and extends its biological half-life. This modification transforms a peptide with a half-life of minutes into one with effective clinical activity lasting weeks to months when formulated in sustained-release preparations.
Contents
Triptorelin has been approved by regulatory agencies in multiple countries for a range of indications, including advanced prostate cancer, endometriosis, uterine fibroids, central precocious puberty, and assisted reproduction. It is marketed under several trade names, including Trelstar (US), Decapeptyl (Europe), and Diphereline (various markets). Among the GnRH agonists, triptorelin is one of the most widely prescribed globally, with decades of clinical experience supporting its safety and efficacy profile.
The peptide’s clinical utility rests on a paradox: while triptorelin initially stimulates the release of gonadotropins (LH and FSH), chronic administration suppresses gonadotropin secretion and reduces sex steroid production to castrate or postmenopausal levels. This biphasic response, initial stimulation followed by sustained suppression, is the hallmark pharmacology of GnRH agonists and forms the basis for their therapeutic applications.
Mechanism of Action
Triptorelin binds to GnRH receptors on gonadotroph cells in the anterior pituitary with approximately 100-fold greater affinity than native GnRH. Upon initial administration, this receptor activation stimulates a surge of LH and FSH release, which in turn produces a transient increase in testosterone (in males) or estradiol (in females). This initial phase is sometimes called the “flare” effect and typically lasts one to two weeks.
With continued exposure to triptorelin, the GnRH receptors on pituitary gonadotrophs undergo downregulation and desensitization. The continuous, non-pulsatile stimulation provided by triptorelin is fundamentally different from the pulsatile GnRH signaling that the pituitary requires for sustained gonadotropin production. Natural GnRH is released in pulses approximately every 60 to 120 minutes, and this intermittent pattern is essential for maintaining GnRH receptor expression and gonadotropin synthesis. When this pulsatility is overridden by continuous agonist exposure, the pituitary reduces its production of LH and FSH, and circulating sex steroid levels fall to levels comparable to surgical castration (in males) or postmenopause (in females).
The molecular events underlying desensitization include receptor internalization, reduced receptor synthesis, uncoupling of the receptor from its downstream signaling pathways, and decreased expression of gonadotropin subunit genes. These changes are reversible: discontinuation of triptorelin allows the restoration of pulsatile GnRH signaling and recovery of gonadal function, typically within several months.
Research Summary
The clinical evidence for triptorelin is extensive, anchored by large randomized controlled trials across multiple indications.
In prostate cancer, triptorelin has been studied in several major trials demonstrating its efficacy in achieving and maintaining castrate testosterone levels (below 50 ng/dL, and in many patients below 20 ng/dL). The sustained-release formulations (one-month, three-month, and six-month depot injections) have been shown to produce reliable testosterone suppression in greater than 95% of patients. Long-term studies have confirmed maintained suppression over treatment periods of years, supporting triptorelin’s use as a standard component of androgen deprivation therapy for advanced prostate cancer.
In endometriosis, controlled trials have demonstrated that triptorelin is as effective as danazol and other GnRH agonists in reducing pelvic pain, dysmenorrhea, and endometriotic lesion size. Treatment courses of three to six months produce significant symptomatic relief, though the hypoestrogenic side effects (hot flashes, vaginal dryness, bone density loss) limit the duration of treatment. “Add-back” therapy with low-dose estrogen and progesterone has been shown to mitigate these side effects while preserving efficacy.
For central precocious puberty, triptorelin depot injections effectively suppress premature pubertal development, slow skeletal maturation, and improve predicted adult height. Studies have shown that treatment is safe and well tolerated in children, with pubertal development resuming normally after discontinuation.
In the context of assisted reproduction, short courses of triptorelin are used in “long protocol” IVF regimens to prevent premature LH surges. The initial flare effect of triptorelin has also been exploited in “flare protocols” designed to recruit additional follicles for oocyte retrieval.
In the peptide research community, triptorelin is sometimes discussed in the context of post-cycle therapy (PCT) for recovery of the hypothalamic-pituitary-gonadal axis following anabolic steroid use. While there is a pharmacological rationale for this application (the initial LH surge could theoretically jumpstart testicular function), this use is not supported by controlled clinical trials and remains off-label.
Dosing in Published Research
About this section
The information below reports dosing only as it appears in published clinical or preclinical research and official regulatory documents. It is provided as published-literature reference material. It is not dosing guidance, not medical advice, and not a recommendation to use or self-administer this compound.
Triptorelin is an FDA-approved prescription medicine, sold as Trelstar. For advanced prostate cancer, the FDA-approved labeling provides depot formulations given by intramuscular injection at fixed intervals:
- 3.75 mg given once monthly.
- 11.25 mg given once every 3 months.
- 22.5 mg given once every 6 months.
These figures are drawn from FDA-approved prescribing information. Triptorelin is also marketed in other formulations for other approved indications.
Important
Triptorelin is a long-acting GnRH agonist; treatment initially causes a transient surge in testosterone before suppression. The depot doses above apply to the approved prescription product administered by a healthcare professional; they are not a recommendation and do not apply to material sold for research use.
Safety and Side Effects
The safety profile of triptorelin is well characterized through extensive clinical use. The most common side effects are direct consequences of sex steroid suppression: hot flashes, decreased libido, erectile dysfunction (in males), vaginal dryness (in females), mood changes, and fatigue. These effects are pharmacologically predictable and generally reversible upon discontinuation.
The initial testosterone/estradiol flare can be clinically significant in certain situations, particularly in prostate cancer patients with bone metastases, where a transient rise in testosterone can cause “flare” symptoms including bone pain and, rarely, spinal cord compression or urinary obstruction. For this reason, anti-androgen therapy is typically co-administered during the first weeks of treatment to block the effects of the testosterone surge.
Long-term GnRH agonist therapy is associated with bone density loss, cardiovascular risk factors (including metabolic syndrome, increased body fat, and unfavorable lipid changes), and cognitive effects. These concerns are most relevant in the context of prolonged androgen deprivation for prostate cancer, where treatment may continue for years. Guidelines recommend monitoring bone density and metabolic parameters in patients on extended therapy.
Injection site reactions (pain, nodules, erythema) occur in a minority of patients receiving depot formulations. Allergic reactions are rare. No carcinogenic effects have been attributed to triptorelin, despite its widespread use in oncology.
Current Research Status
Triptorelin is an approved pharmaceutical with well-established clinical indications. It is marketed globally and included in major clinical practice guidelines for prostate cancer, endometriosis, uterine fibroids, central precocious puberty, and assisted reproduction. Current research is exploring optimized dosing strategies, combination therapies in oncology, and comparative effectiveness studies against newer GnRH antagonists (such as degarelix), which achieve gonadal suppression without the initial flare effect. Triptorelin remains one of the most clinically validated peptides in the entire pharmacopeia.
Frequently Asked Questions
What is triptorelin?
Triptorelin is a synthetic decapeptide analog of gonadotropin-releasing hormone (GnRH), the hormone that controls the body’s sex-hormone system. It is an FDA-approved prescription medicine, sold as Trelstar and other brands, used mainly for advanced prostate cancer and certain other hormone-related conditions.
How does triptorelin work?
Triptorelin binds GnRH receptors in the pituitary with much greater affinity than natural GnRH. Initial dosing causes a brief surge in LH, FSH and sex hormones, but continuous stimulation then desensitizes the receptors, ultimately suppressing testosterone or estrogen.
Is triptorelin FDA-approved?
Yes. Triptorelin is an FDA-approved pharmaceutical with well-established indications, marketed globally and included in major clinical guidelines for prostate cancer, endometriosis, uterine fibroids, central precocious puberty and assisted reproduction.
What does the research say about triptorelin?
The clinical evidence is extensive, anchored by large randomized controlled trials. In prostate cancer, multiple major trials have shown triptorelin achieves and maintains castrate testosterone levels, and it has documented data across its other approved indications.
What are the safety concerns with triptorelin?
The most common side effects are direct consequences of sex steroid suppression: hot flashes, decreased libido, erectile dysfunction in males, vaginal dryness in females, mood changes and fatigue. There is also a transient hormonal surge when treatment begins.
Research Handling & Storage
Reconstitution (General Guidelines)
Lyophilized peptides are typically reconstituted using bacteriostatic water (0.9% benzyl alcohol). Standard reconstitution protocol:
- Remove the vial from storage and allow it to reach room temperature (20–25°C / 68–77°F) before opening. This typically takes 15–20 minutes.
- Clean the vial stopper with an alcohol prep pad and allow to air dry.
- Using a sterile syringe, slowly inject bacteriostatic water along the inside wall of the vial. Do not spray directly onto the lyophilized powder.
- Gently swirl the vial until the powder is fully dissolved. Do not shake vigorously as this may damage the peptide structure.
- The reconstituted solution should be clear and colorless. Discard if cloudy, discolored, or if particulate matter is visible.
- Label the vial with the reconstitution date, concentration, and your initials.
Common reconstitution volumes in research: 1ml or 2ml of bacteriostatic water per vial, depending on the desired concentration. For example, adding 2ml to a 5mg vial yields a concentration of 2.5mg/ml (2,500mcg/ml).
Storage
- Lyophilized (unreconstituted): Store at -20°C (-4°F) for long-term storage (stable 24+ months), or 2–8°C (36–46°F) refrigerated for short-term storage up to 6 months. Keep desiccated and protected from light.
- Reconstituted: Store at 2–8°C (36–46°F) refrigerated. Use within 4–6 weeks of reconstitution. Do not freeze reconstituted solutions as this may cause degradation.
- Shipping: Lyophilized peptides are generally stable at ambient temperature during transit for several days. Reconstituted solutions should be shipped on ice packs.
Handling Precautions
- Handle with appropriate personal protective equipment (PPE) including nitrile gloves, lab coat, and eye protection.
- Use aseptic/sterile technique when reconstituting and transferring solutions to prevent contamination.
- Avoid repeated freeze-thaw cycles which may denature the compound and reduce potency.
- Keep detailed laboratory records including reconstitution dates, lot numbers, concentrations, and storage conditions.
- Dispose of unused material and sharps in accordance with local regulations and institutional biosafety guidelines.
Stability & Shelf Life
Lyophilized (freeze-dried) peptides are highly stable when stored correctly. At -20°C (-4°F), most peptides retain >95% purity for 24 months or longer. Once reconstituted, the clock starts—proteins in solution are inherently less stable than in dry form. Factors that accelerate degradation include temperature fluctuations, exposure to light, repeated freeze-thaw cycles, bacterial contamination, and oxidation.
Purity & Quality Considerations
Research-grade compounds should be accompanied by a Certificate of Analysis (COA) confirming purity, typically verified by High-Performance Liquid Chromatography (HPLC) and Mass Spectrometry (MS). Look for purity levels of ≥98% for research applications. Third-party testing adds an additional layer of quality assurance. Always verify the source and documentation before using any research compound.
Research Supplies & Resources
Essential supplies and educational resources for peptide research. Links go to Amazon.com.
Lab Supplies
Recommended Reading
Lab Equipment
As an Amazon Associate, peptides.fyi earns from qualifying purchases. Learn more.