Synopsis
Compound overview
- Research only
- In clinical trials
- Approved outside US
- FDA-approved
What it is
Cabergoline is a dopamine agonist. It is an FDA-approved prescription medicine, used mainly to treat conditions caused by too much of the hormone prolactin.
What it does
Documented and off-label uses include:
- Lowers high prolactin levels
- Treats prolactin-secreting pituitary tumours
- Used off the research scene to manage prolactin side effects
- Long-acting, taken once or twice weekly
How it works
Cabergoline activates dopamine receptors, and dopamine naturally suppresses prolactin release from the pituitary gland — so the drug brings high prolactin levels back down.
Safety notes
Cabergoline is prescription-only. High doses, mainly in other dopamine-agonist uses, have been linked to heart-valve problems, and it can cause nausea, dizziness and low blood pressure on standing. It should be used under medical supervision; research-vendor material is not pharmacy-grade.
Where to buy Cabergoline
Standard lyophilized vial — reconstitute and measure doses yourself. The conventional research format.
Affiliate links — we may earn a commission at no extra cost to you.
Molecular Structure
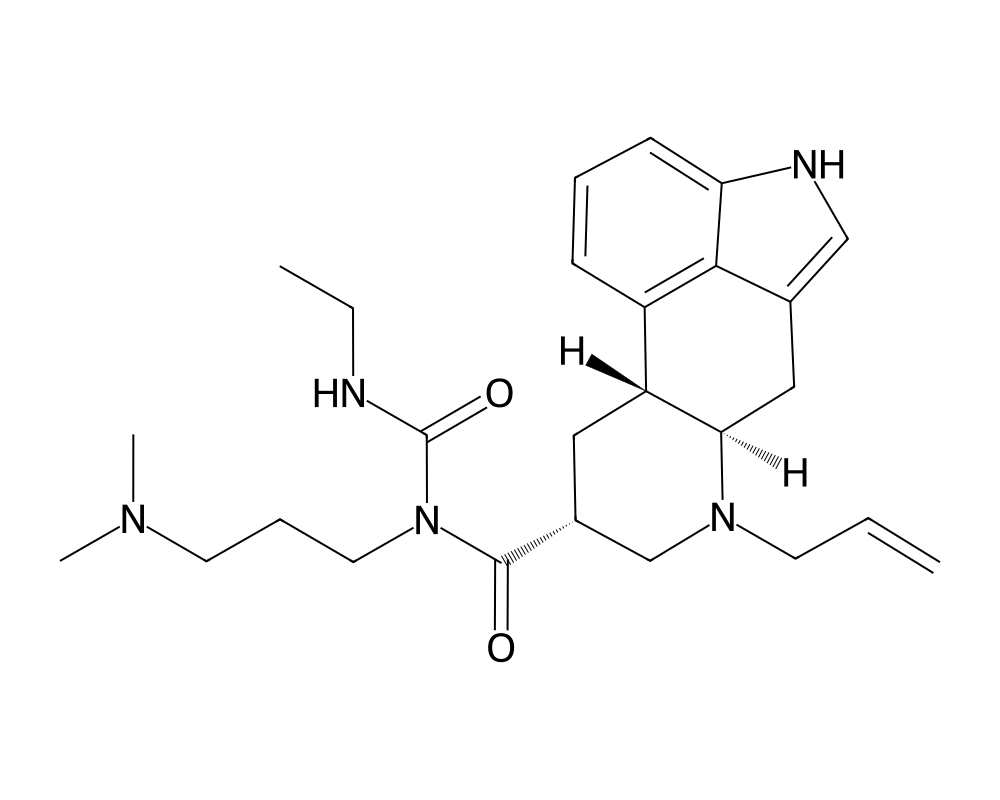
Overview
Cabergoline is a long-acting dopamine receptor agonist derived from the ergot alkaloid family. Originally developed by Pharmacia (now part of Pfizer) and marketed under the brand name Dostinex, it received FDA approval in 1996 for the treatment of hyperprolactinemia, a condition characterized by abnormally elevated levels of the hormone prolactin. The compound has since become the first-line pharmacological treatment for prolactin-secreting pituitary adenomas (prolactinomas), displacing the older dopamine agonist bromocriptine in most clinical settings due to superior efficacy and tolerability.
Contents
Cabergoline is distinguished from earlier dopamine agonists by its extended pharmacokinetic profile. A single oral dose produces therapeutic effects lasting up to seven days, allowing for twice-weekly dosing in most patients. This extended duration of action stems from the compound’s high binding affinity for dopamine D2 receptors and its slow elimination from the body, with a terminal half-life estimated between 63 and 69 hours. For researchers studying prolactin physiology, dopaminergic signaling, and pituitary function, cabergoline serves as both a clinical tool and a pharmacological probe.
Mechanism of Action
Cabergoline exerts its primary pharmacological effect through potent and selective agonism at dopamine D2 receptors on lactotroph cells in the anterior pituitary gland. Prolactin secretion is unique among pituitary hormones in that it is primarily under tonic inhibitory control by hypothalamic dopamine. When dopamine binds to D2 receptors on lactotrophs, it suppresses prolactin gene transcription, inhibits prolactin release, and reduces lactotroph cell proliferation.
By mimicking dopamine at these receptor sites, cabergoline effectively suppresses prolactin synthesis and secretion, often normalizing serum prolactin levels within weeks of initiation. In the context of prolactinomas, the compound not only reduces prolactin output but also induces tumor shrinkage in a majority of patients, sometimes dramatically. This dual effect on hormone secretion and tumor mass makes it a compelling subject for researchers investigating pituitary adenoma biology.
Beyond D2 receptor agonism, cabergoline displays weak affinity for D1, D3, and D4 dopamine receptors, as well as serotonin 5-HT2B receptors. The 5-HT2B activity has clinical significance: chronic stimulation of cardiac 5-HT2B receptors is associated with valvular heart disease, a concern that emerged from studies of other ergot-derived dopamine agonists used at high doses in Parkinson’s disease. At the lower doses used for hyperprolactinemia, this risk appears minimal, though it remains a subject of ongoing research.
Research Summary
The clinical evidence base for cabergoline is extensive. Landmark studies published in the 1990s and 2000s established its superiority over bromocriptine for normalizing prolactin levels, with response rates exceeding 80% in patients with idiopathic hyperprolactinemia and microprolactinomas. Macroprolactinomas, which are more challenging to manage, still showed response rates above 70% in large case series.
Tumor shrinkage data are particularly striking. In a meta-analysis of published studies, cabergoline produced significant tumor volume reduction in approximately 80% of macroprolactinoma patients, with some tumors decreasing by more than 50% within the first three months of treatment. Long-term follow-up studies have demonstrated sustained tumor control over periods exceeding 10 years in many patients.
Research into cabergoline withdrawal has yielded encouraging findings. Studies have shown that after at least two years of treatment, a substantial proportion of patients (ranging from 30% to 70% depending on the study) can discontinue the drug without prolactin recurrence, particularly those with idiopathic hyperprolactinemia or small tumors. This has led to the development of withdrawal protocols now used in clinical practice.
In the research community studying performance enhancement, cabergoline has attracted interest for its ability to suppress prolactin elevations that can occur with certain anabolic compounds, particularly 19-nortestosterone derivatives like nandrolone and trenbolone. Elevated prolactin in these contexts can produce gynecomastia, sexual dysfunction, and mood disturbances. While this application lacks formal clinical trial support, the pharmacological rationale is well-grounded in dopamine-prolactin physiology.
Dosing in Published Research
About this section
The information below reports dosing only as it appears in published clinical or preclinical research and official regulatory documents. It is provided as published-literature reference material. It is not dosing guidance, not medical advice, and not a recommendation to use or self-administer this compound.
Cabergoline is an FDA-approved prescription medicine, sold as Dostinex. For hyperprolactinemic disorders, the FDA-approved labeling specifies a titrated schedule:
- Start at 0.25 mg taken twice weekly.
- Increase by 0.25 mg twice weekly, at intervals of at least 4 weeks, to normalize serum prolactin.
- The labeled maximum is 1 mg twice weekly.
These figures are drawn from FDA-approved prescribing information.
Important
Cabergoline has been associated with cardiac valve disease, particularly with the higher and prolonged dosing used for Parkinson disease. The schedule above applies to the approved prescription product used under medical supervision; it is not a recommendation and does not apply to material sold for research use.
Safety and Side Effects
At standard doses for hyperprolactinemia (typically 0.25 to 1.0 mg twice weekly), cabergoline is generally well tolerated. The most common adverse effects include nausea, headache, dizziness, and fatigue, which tend to be mild and often diminish with continued use. Orthostatic hypotension can occur, particularly at treatment initiation, and is managed by starting with low doses taken at bedtime.
The cardiac valvulopathy concern deserves careful consideration. Studies of Parkinson’s disease patients taking cabergoline at doses of 3 to 6 mg daily (several times the doses used for hyperprolactinemia) showed increased rates of clinically significant valve regurgitation, particularly tricuspid and mitral. However, multiple echocardiographic studies of hyperprolactinemia patients on standard doses have not demonstrated increased valvular disease risk. Current guidelines nonetheless recommend baseline and periodic echocardiographic monitoring.
Impulse control disorders, including pathological gambling, hypersexuality, and compulsive spending, have been reported with dopamine agonists as a class. While the incidence appears lower with cabergoline than with the non-ergot agonists used in Parkinson’s disease, researchers and clinicians should remain vigilant for these behavioral changes. Rare cases of cerebrospinal fluid rhinorrhea have been reported in patients with large invasive prolactinomas undergoing rapid tumor shrinkage.
Current Research Status
Cabergoline is an FDA-approved medication with a well-established clinical track record spanning nearly three decades. Current research efforts focus on optimizing treatment duration and withdrawal protocols, understanding long-term cardiovascular safety at various dose ranges, and exploring potential applications beyond hyperprolactinemia. Investigators are examining the compound’s effects on metabolic parameters, given the relationship between hyperprolactinemia and insulin resistance. Additionally, research continues into the use of cabergoline for ovarian hyperstimulation syndrome prevention and as adjunctive therapy in certain psychiatric conditions involving dopaminergic dysfunction.
Frequently Asked Questions
What is cabergoline?
Cabergoline is a long-acting dopamine agonist derived from the ergot alkaloid family. Marketed as Dostinex, it is an FDA-approved prescription medicine, approved in 1996, used mainly for conditions caused by excess prolactin.
How does cabergoline work?
Cabergoline activates dopamine D2 receptors on lactotroph cells in the pituitary gland. Because dopamine naturally suppresses prolactin release, this lowers prolactin levels. Its long duration of action allows once- or twice-weekly dosing.
Is cabergoline FDA-approved?
Yes. Cabergoline is an FDA-approved medication with a clinical track record spanning nearly three decades, used mainly for hyperprolactinemia and prolactin-secreting pituitary tumors.
What does the research say about cabergoline?
Landmark studies established cabergoline’s superiority over bromocriptine for normalizing prolactin, with response rates exceeding 80% in idiopathic hyperprolactinemia and microprolactinomas. Long-term cardiovascular safety at various doses remains an area of study.
What are the safety concerns with cabergoline?
At standard doses for hyperprolactinemia, cabergoline is generally well tolerated; common side effects include nausea, headache, dizziness and fatigue, often mild. Orthostatic hypotension can occur, and high-dose use has prompted study of possible cardiac valve effects.
Research Handling & Storage
Storage
- Unopened: Store at controlled room temperature, 20–25°C (68–77°F), away from direct sunlight, heat, and moisture.
- Opened: Keep container tightly closed. Use within the timeframe indicated on the label, typically 30–90 days after opening.
- Do not freeze liquid solutions unless specifically indicated.
Handling Precautions
- Handle with appropriate personal protective equipment (PPE) including nitrile gloves, lab coat, and eye protection.
- Use aseptic/sterile technique when reconstituting and transferring solutions to prevent contamination.
- Avoid repeated freeze-thaw cycles which may denature the compound and reduce potency.
- Keep detailed laboratory records including reconstitution dates, lot numbers, concentrations, and storage conditions.
- Dispose of unused material and sharps in accordance with local regulations and institutional biosafety guidelines.
Stability & Shelf Life
Liquid formulations typically remain stable for 1–2 years when stored at the recommended temperature in the original sealed container. Once opened, potency may gradually decrease. Monitor for any changes in color, clarity, or odor, which may indicate degradation.
Purity & Quality Considerations
Research-grade compounds should be accompanied by a Certificate of Analysis (COA) confirming purity, typically verified by High-Performance Liquid Chromatography (HPLC) and Mass Spectrometry (MS). Look for purity levels of ≥98% for research applications. Third-party testing adds an additional layer of quality assurance. Always verify the source and documentation before using any research compound.
Research Supplies & Resources
Essential supplies and educational resources for peptide research. Links go to Amazon.com.
Lab Supplies
Recommended Reading
Lab Equipment
As an Amazon Associate, peptides.fyi earns from qualifying purchases. Learn more.