Synopsis
Compound overview
- Research only
- In clinical trials
- Approved outside US
- FDA-approved
What it is
AICAR (acadesine) is a compound that activates AMPK, a master regulator of cellular energy. It has been studied in clinical trials — for example in heart surgery and certain blood cancers — but it is not an approved drug.
What it does
How it has been studied and marketed:
- Studied for effects on endurance and metabolism
- Investigated in heart-surgery and cancer trials
- Promoted (illegally) as an "exercise mimetic"
- Banned in all competitive sport
How it works
AICAR switches on AMPK, an enzyme cells use to sense low energy. Activating it pushes cells toward burning fuel and building energy capacity, which is the basis for the "exercise in a pill" idea.
Safety notes
Despite being studied in trials, AICAR is not an approved medicine and must be injected, since it is poorly absorbed by mouth. It can disturb uric-acid levels and metabolism, and research-grade purity varies. It is banned in sport, and any non-trial use is experimental.
Where to buy AICAR
Standard lyophilized vial — reconstitute and measure doses yourself. The conventional research format.
Affiliate links — we may earn a commission at no extra cost to you.
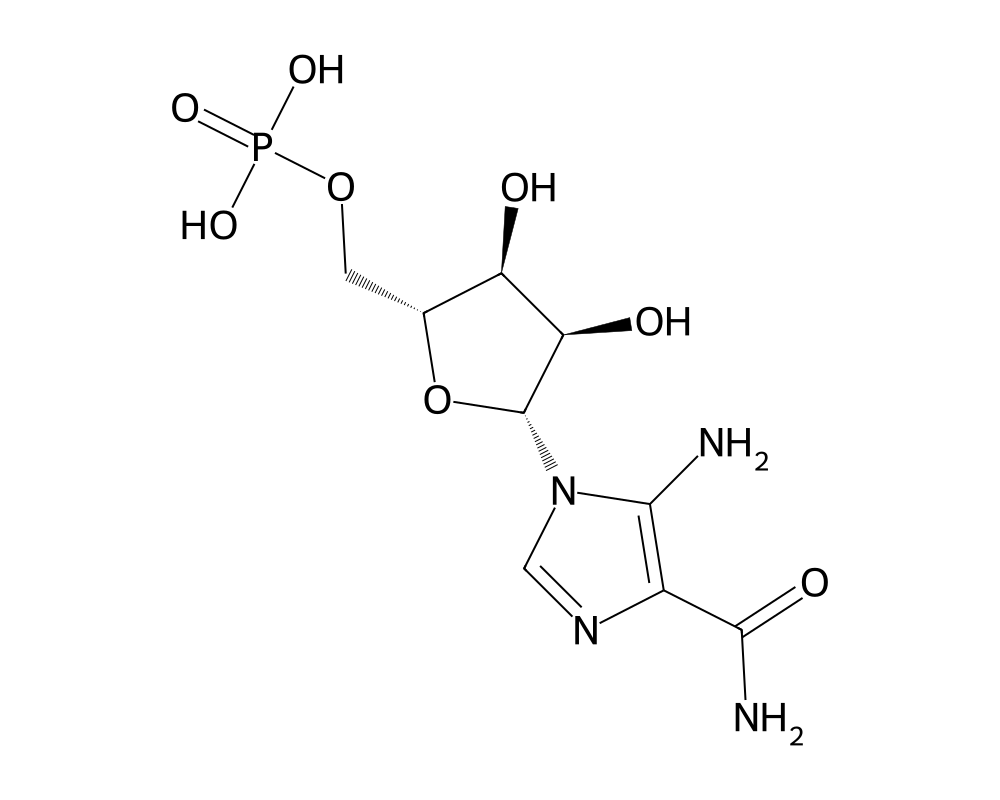
Molecular Structure
Research tool
Reconstitution calculator
Concentration
2.50mg/mL
Draw volume
0.10mL
Insulin units
10IU
Doses/vial
20
Overview
AICAR (5-aminoimidazole-4-carboxamide ribonucleoside, also known as acadesine) is a nucleoside analog that has gained prominence as a pharmacological activator of AMP-activated protein kinase (AMPK), one of the most important metabolic regulatory enzymes in biology. Strictly speaking, AICAR is not a peptide. It is a small molecule nucleoside. However, it is frequently discussed alongside peptides in performance and metabolic research communities because of its overlapping applications and its inclusion in the same regulatory and anti-doping frameworks that govern many research peptides.
Contents
AICAR occurs naturally in the body as an intermediate in the de novo purine biosynthesis pathway. When administered exogenously at pharmacological doses, it is taken up by cells and phosphorylated by adenosine kinase to form ZMP (AICAR monophosphate), which mimics the effects of AMP (adenosine monophosphate) on AMPK. This activation of AMPK triggers a broad cascade of metabolic effects that mimic exercise, caloric restriction, and other states of energy deficit, earning AICAR the label of “exercise in a pill” in popular media coverage.
The compound was originally developed for cardiovascular applications, specifically for reducing ischemic injury during cardiac surgery. It was investigated in Phase III clinical trials for this indication in the 1990s under the name acadesine. While it did not ultimately receive FDA approval, the cardiovascular research produced extensive safety and pharmacological data in humans. More recently, AICAR has attracted attention for its effects on endurance performance, fat metabolism, and the molecular pathways associated with exercise adaptation.
Mechanism of Action
AICAR’s pharmacological effects center on the activation of AMPK. After cellular uptake and phosphorylation to ZMP, the molecule binds to the gamma subunit of AMPK, mimicking the allosteric activation normally triggered by rising AMP levels during states of energy depletion. AMPK activation produces a coordinated metabolic response that prioritizes energy-generating catabolic pathways and suppresses energy-consuming anabolic processes.
The downstream effects of AMPK activation are extensive. In skeletal muscle, AMPK stimulates glucose uptake (independent of insulin, through GLUT4 translocation), enhances fatty acid oxidation (by phosphorylating and inhibiting acetyl-CoA carboxylase, which reduces malonyl-CoA and relieves inhibition of carnitine palmitoyltransferase 1), and promotes mitochondrial biogenesis (through activation of PGC-1 alpha, a master regulator of mitochondrial gene expression). These are the same adaptations that occur with endurance exercise training, which is why AICAR-induced AMPK activation mimics many aspects of exercise at the molecular level.
In the liver, AMPK activation suppresses gluconeogenesis and lipogenesis, reducing hepatic glucose output and fat synthesis. In adipose tissue, AMPK inhibits lipolysis at moderate activation levels but can stimulate fatty acid oxidation. The net metabolic effect is improved insulin sensitivity, enhanced fat utilization, and reduced lipid accumulation.
AMPK also modulates inflammatory signaling, inhibiting NF-kB-mediated pro-inflammatory gene expression. This anti-inflammatory activity has implications for conditions ranging from atherosclerosis to neurodegeneration.
In the cardiovascular system, AICAR’s effects during ischemia involve both AMPK-dependent and AMPK-independent mechanisms. The compound is converted to inosine monophosphate (IMP) and ultimately to adenosine, a potent vasodilator and cardioprotective agent. AICAR also inhibits adenosine deaminase, increasing local adenosine concentrations. These adenosine-related effects were the basis for the original cardiovascular development program.
Research Summary
The research base for AICAR is extensive, spanning basic science, preclinical studies, and human clinical trials.
The landmark study that propelled AICAR into public awareness was published in Cell in 2008 by Ronald Evans and colleagues at the Salk Institute. This study demonstrated that AICAR administration to sedentary mice for four weeks improved running endurance by 44 percent without any exercise training. The mice showed metabolic gene expression patterns in skeletal muscle that closely resembled those of trained animals, including upregulation of oxidative metabolism genes and mitochondrial biogenesis markers. This finding generated widespread media coverage and prompted WADA (the World Anti-Doping Agency) to add AICAR to its prohibited substances list in 2009.
Subsequent animal studies confirmed and extended these findings. AICAR treatment has been shown to increase the proportion of type I (slow-twitch, oxidative) muscle fibers, enhance endurance capacity, reduce body fat, improve glucose tolerance, and protect against diet-induced obesity in rodent models. In aged mice, AICAR treatment improved physical performance and extended healthy lifespan markers, consistent with the known association between AMPK activity and longevity pathways.
The cardiovascular clinical program produced the largest body of human data. The AMISTAD (Acadesine Myocardial Ischemia Study During Angioplasty and Bypass) trials enrolled thousands of patients undergoing coronary artery bypass surgery. AMISTAD I showed a trend toward reduced myocardial infarction, stroke, and death with acadesine treatment, though the primary endpoint was not statistically significant. AMISTAD II was terminated early for futility, dampening enthusiasm for the cardiovascular indication. However, these trials demonstrated that AICAR can be administered intravenously to humans at pharmacological doses with acceptable safety.
Metabolic disease research continues to explore AICAR as a potential treatment for type 2 diabetes and metabolic syndrome. The compound’s ability to improve glucose uptake independent of insulin makes it theoretically attractive for patients with insulin resistance. However, the requirement for parenteral administration (AICAR has poor oral bioavailability) and its broad metabolic effects have complicated drug development for this indication.
Anti-doping authorities have developed testing methods for AICAR, and several athletes have been investigated for its use. The challenge of distinguishing exogenous AICAR from endogenous levels (since it is a natural metabolic intermediate) has been a technical hurdle for anti-doping laboratories.
Dosing in Published Research
About this section
The information below reports dosing only as it appears in published clinical or preclinical research and official regulatory documents. It is provided as published-literature reference material. It is not dosing guidance, not medical advice, and not a recommendation to use or self-administer this compound.
AICAR (also studied as acadesine) is an AMP-activated protein kinase activator. It is not an approved medicine and has no labeled dose. It has been given in human trials by intravenous infusion, because of poor oral absorption; across those studies single-dose infusions have spanned a wide range, with figures up to roughly 210 mg per kilogram of body weight reported as tolerated in short-term use. These figures describe what was administered in those specific trials.
Research doses, not a protocol
These are intravenous research doses used in supervised clinical studies, not an established or recommended regimen, and AICAR is poorly absorbed when taken by mouth. It is not an approved drug, is prohibited in sport by WADA, and material sold for research use is not a regulated drug product.
Safety and Side Effects
Human safety data for AICAR come primarily from the cardiovascular clinical trials, in which the compound was administered as an intravenous infusion during and after cardiac surgery. In these studies, the most common side effects were transient hypoglycemia, hyperuricemia (elevated uric acid, a predictable consequence of purine metabolism), and bradycardia. These effects were generally manageable and dose-related.
Hypoglycemia is a direct consequence of AMPK-mediated glucose uptake and requires monitoring, particularly when AICAR is used in conjunction with other glucose-lowering agents or in fasting states. The hyperuricemia results from the metabolism of AICAR through purine pathways and could theoretically precipitate gout in susceptible individuals.
Long-term safety data are limited. The cardiovascular trials involved acute, short-term administration (hours to days), and the effects of chronic AICAR use over weeks or months in humans are not well characterized. Preclinical data suggest that chronic AMPK activation could potentially interfere with cardiac hypertrophy responses (AMPK inhibits mTOR-dependent growth pathways), which could be detrimental in contexts where cardiac adaptation is needed.
Because AICAR is a nucleoside analog, theoretical concerns about genotoxicity have been raised, though standard genotoxicity assays conducted during clinical development did not reveal significant mutagenic potential. No carcinogenic effects have been observed in animal studies.
Renal effects require consideration, as AICAR is cleared primarily through the kidneys. Dose adjustment or caution may be warranted in patients with renal impairment.
Current Research Status
AICAR is not approved by any regulatory agency for clinical use. Its cardiovascular development program was discontinued after the AMISTAD II trial results. The compound is available as a research chemical and is listed on WADA’s prohibited substances list for athletic competition. Current research interests include metabolic disease, exercise physiology, longevity, neurodegenerative disease, and cancer (where AMPK activation can suppress tumor cell growth in some contexts). The development of orally bioavailable AMPK activators by pharmaceutical companies may ultimately supersede AICAR for therapeutic applications, but the compound remains the most widely used pharmacological AMPK activator in laboratory research.
Frequently Asked Questions
What is AICAR?
AICAR, also called acadesine, is a nucleoside analog that acts as a pharmacological activator of AMP-activated protein kinase (AMPK), a master regulator of cellular energy. It has been studied in clinical trials but is not an approved drug.
How does AICAR work?
After cellular uptake, AICAR is converted to a metabolite (ZMP) that binds AMPK, mimicking the activation normally triggered by low cellular energy. AMPK activation shifts cells toward energy production and altered metabolism.
Is AICAR FDA-approved?
No. AICAR is not approved by any regulatory agency for clinical use. Its cardiovascular development program was discontinued, and it is on WADA’s prohibited substances list for athletic competition.
What does the research say about AICAR?
A widely cited 2008 study in Cell by Evans and colleagues showed AICAR altered endurance and metabolism in mice, which drew public attention. It has also been investigated in heart-surgery and blood-cancer trials, though the cardiac program was discontinued after the AMISTAD II trial.
What are the safety concerns with AICAR?
Human safety data come mainly from cardiovascular trials, where AICAR was given as an intravenous infusion during cardiac surgery. The most common side effects were transient low blood sugar and elevated uric acid. Long-term safety outside that setting is not established.
Research Handling & Storage
Reconstitution (General Guidelines)
Lyophilized peptides are typically reconstituted using bacteriostatic water (0.9% benzyl alcohol). Standard reconstitution protocol:
- Remove the vial from storage and allow it to reach room temperature (20–25°C / 68–77°F) before opening. This typically takes 15–20 minutes.
- Clean the vial stopper with an alcohol prep pad and allow to air dry.
- Using a sterile syringe, slowly inject bacteriostatic water along the inside wall of the vial. Do not spray directly onto the lyophilized powder.
- Gently swirl the vial until the powder is fully dissolved. Do not shake vigorously as this may damage the peptide structure.
- The reconstituted solution should be clear and colorless. Discard if cloudy, discolored, or if particulate matter is visible.
- Label the vial with the reconstitution date, concentration, and your initials.
Common reconstitution volumes in research: 1ml or 2ml of bacteriostatic water per vial, depending on the desired concentration. For example, adding 2ml to a 5mg vial yields a concentration of 2.5mg/ml (2,500mcg/ml).
Storage
- Lyophilized (unreconstituted): Store at -20°C (-4°F) for long-term storage (stable 24+ months), or 2–8°C (36–46°F) refrigerated for short-term storage up to 6 months. Keep desiccated and protected from light.
- Reconstituted: Store at 2–8°C (36–46°F) refrigerated. Use within 4–6 weeks of reconstitution. Do not freeze reconstituted solutions as this may cause degradation.
- Shipping: Lyophilized peptides are generally stable at ambient temperature during transit for several days. Reconstituted solutions should be shipped on ice packs.
Handling Precautions
- Handle with appropriate personal protective equipment (PPE) including nitrile gloves, lab coat, and eye protection.
- Use aseptic/sterile technique when reconstituting and transferring solutions to prevent contamination.
- Avoid repeated freeze-thaw cycles which may denature the compound and reduce potency.
- Keep detailed laboratory records including reconstitution dates, lot numbers, concentrations, and storage conditions.
- Dispose of unused material and sharps in accordance with local regulations and institutional biosafety guidelines.
Stability & Shelf Life
Lyophilized (freeze-dried) peptides are highly stable when stored correctly. At -20°C (-4°F), most peptides retain >95% purity for 24 months or longer. Once reconstituted, the clock starts—proteins in solution are inherently less stable than in dry form. Factors that accelerate degradation include temperature fluctuations, exposure to light, repeated freeze-thaw cycles, bacterial contamination, and oxidation.
Purity & Quality Considerations
Research-grade compounds should be accompanied by a Certificate of Analysis (COA) confirming purity, typically verified by High-Performance Liquid Chromatography (HPLC) and Mass Spectrometry (MS). Look for purity levels of ≥98% for research applications. Third-party testing adds an additional layer of quality assurance. Always verify the source and documentation before using any research compound.
Research Supplies & Resources
Essential supplies and educational resources for peptide research. Links go to Amazon.com.
Lab Supplies
Recommended Reading
Lab Equipment
As an Amazon Associate, peptides.fyi earns from qualifying purchases. Learn more.