Synopsis
Compound overview
- Research only
- In clinical trials
- Approved outside US
- FDA-approved
What it is
Clomiphene (Clomid) is a selective estrogen receptor modulator (SERM). It is an FDA-approved prescription medicine, used mainly to treat infertility in women by stimulating ovulation.
What it does
Documented and off-label uses include:
- Stimulates ovulation in fertility treatment
- Raises the body's own reproductive hormones
- Used off-label by some men to raise testosterone
- Has long-standing clinical data
How it works
Clomiphene blocks estrogen receptors in the brain, which the body reads as low estrogen. It responds by releasing more FSH and LH — hormones that drive ovulation in women and testosterone production in men.
Safety notes
Clomiphene is prescription-only and used under medical supervision. Side effects include hot flushes, mood changes and visual disturbances, and in fertility treatment it raises the chance of multiple pregnancy. Self-directed use without monitoring is not safe, and research-vendor material is not pharmacy-grade.
Where to buy Clomiphene Citrate
Standard lyophilized vial — reconstitute and measure doses yourself. The conventional research format.
Affiliate links — we may earn a commission at no extra cost to you.
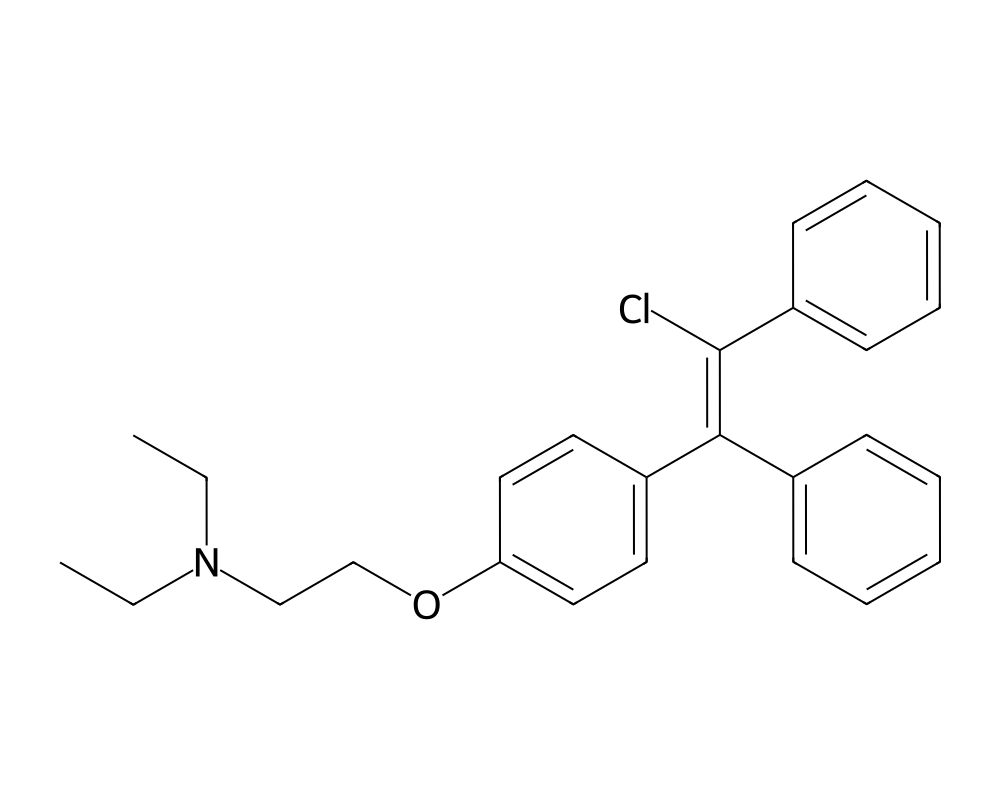
Molecular Structure
Overview
Clomiphene citrate is one of the oldest and most extensively studied selective estrogen receptor modulators (SERMs), first synthesized in 1956 and approved by the FDA in 1967 for the treatment of ovulatory dysfunction in women desiring pregnancy. Marketed under the brand names Clomid and Serophene, it has remained a first-line therapy for anovulatory infertility for over five decades, a testament to its efficacy, safety profile, and favorable cost-effectiveness ratio.
Contents
- Overview
- Mechanism of Action
- Hypothalamic-Pituitary Axis Stimulation
- Ovarian Stimulation in Women
- Testosterone Stimulation in Men
- Research Summary
- Early Clinical Development
- Male Hypogonadism Applications
- Comparative Efficacy and Safety
- Dosing in Published Research
- Safety and Side Effects
- Current Research Status
- Frequently Asked Questions
Clomiphene is a racemic mixture of two geometric isomers: enclomiphene (trans-clomiphene) and zuclomiphene (cis-clomiphene), present in an approximately 62:38 ratio in the commercial preparation. These isomers have distinct pharmacological properties: enclomiphene is primarily an estrogen receptor antagonist with a shorter half-life (approximately 10 hours), while zuclomiphene exhibits mixed agonist-antagonist activity with a substantially longer half-life (up to several weeks). The composite pharmacological effect of the racemic mixture reflects the combined actions of both isomers.
Beyond its established role in female infertility, clomiphene has been increasingly studied and used off-label for the treatment of male hypogonadism. By blocking estrogen-mediated negative feedback at the hypothalamic-pituitary level, clomiphene stimulates increased gonadotropin secretion, leading to enhanced testicular testosterone production while preserving spermatogenesis, a critical advantage over exogenous testosterone replacement therapy.
Mechanism of Action
Clomiphene exerts its primary therapeutic effect through competitive antagonism of estrogen receptors in the hypothalamus and anterior pituitary gland. By occupying estrogen receptors in these tissues, clomiphene prevents endogenous estradiol from exerting its normal negative feedback on gonadotropin-releasing hormone (GnRH) and gonadotropin secretion.
Hypothalamic-Pituitary Axis Stimulation
Under normal physiological conditions, circulating estradiol provides tonic negative feedback to hypothalamic GnRH-secreting neurons and pituitary gonadotrope cells, modulating the frequency and amplitude of GnRH pulses and the subsequent release of luteinizing hormone (LH) and follicle-stimulating hormone (FSH). Clomiphene blocks this feedback loop by occupying hypothalamic estrogen receptors, effectively creating a state of perceived estrogen deficiency. The hypothalamus responds by increasing GnRH pulse frequency and amplitude, which in turn stimulates increased pituitary secretion of both LH and FSH.
Ovarian Stimulation in Women
The elevated FSH levels resulting from clomiphene’s hypothalamic blockade promote recruitment and maturation of ovarian follicles in anovulatory women. As follicles develop and produce increasing amounts of estradiol, the midcycle LH surge is triggered (either spontaneously or by the rising estradiol), leading to ovulation. The standard protocol involves administration of 50-150 mg daily for 5 days, beginning on cycle day 3 or 5, with ovulation typically occurring 5-12 days after the last dose.
Testosterone Stimulation in Men
In hypogonadal men, clomiphene’s blockade of hypothalamic estrogen feedback results in increased LH secretion, which stimulates Leydig cell testosterone production. Unlike exogenous testosterone, this mechanism preserves or even enhances intratesticular testosterone concentrations, maintaining the hormonal milieu necessary for ongoing spermatogenesis. Studies have demonstrated that clomiphene can raise serum testosterone levels by 100-200% from baseline in hypogonadal men while maintaining or improving sperm parameters.
Research Summary
Early Clinical Development
Greenblatt et al. (1961) published the foundational clinical study demonstrating clomiphene’s efficacy in inducing ovulation in anovulatory women. This landmark work, published in the Journal of the American Medical Association, established the basic clinical framework for clomiphene therapy that remains largely unchanged today. The study demonstrated ovulation rates of approximately 70-80% and pregnancy rates of 30-40% per treatment cycle in properly selected patients.
Male Hypogonadism Applications
Katz et al. (2012) published a comprehensive review in the BJU International evaluating clomiphene citrate for male hypogonadism and infertility. The analysis of available studies demonstrated that clomiphene therapy in hypogonadal men produced significant increases in serum testosterone (mean increases from approximately 250-350 ng/dL to 500-700 ng/dL), while maintaining or improving semen parameters. This contrasts sharply with exogenous testosterone therapy, which typically suppresses spermatogenesis through negative feedback on the hypothalamic-pituitary-gonadal axis.
Comparative Efficacy and Safety
Multiple randomized controlled trials and meta-analyses have confirmed clomiphene’s position as the first-line pharmacological therapy for anovulatory infertility due to WHO Group II anovulation (including polycystic ovary syndrome). Overall ovulation rates range from 60-85%, with cumulative pregnancy rates of approximately 50-60% over 6 treatment cycles. The drug is generally well tolerated, with the most common side effects being hot flashes, visual disturbances, mood changes, and ovarian hyperstimulation. The risk of multiple gestation is approximately 5-8%, predominantly twins.
Dosing in Published Research
About this section
The information below reports dosing only as it appears in published clinical or preclinical research and official regulatory documents. It is provided as published-literature reference material. It is not dosing guidance, not medical advice, and not a recommendation to use or self-administer this compound.
Clomiphene citrate is an FDA-approved prescription medicine, sold as Clomid. The FDA-approved labeling describes its use for ovulation induction in women:
- First cycle: 50 mg daily for 5 days.
- If ovulation does not occur: a subsequent course of 100 mg daily for 5 days may be used.
- Treatment is generally limited to about six cycles.
These figures are drawn from FDA-approved prescribing information. Use of clomiphene in men, for example for hypogonadism, is off-label and is not described by this labeling.
Important
The regimen above is the labeled protocol for ovulation induction in women and is administered with physician monitoring for ovarian response and ovarian enlargement. It is not a recommendation, and it does not apply to material sold for laboratory or research use.
Safety and Side Effects
Clomiphene is an FDA-approved drug with a long-characterized safety profile. Common adverse effects include hot flashes, mood changes, headache, breast tenderness, and abdominal discomfort. A distinctive and clinically important effect is visual disturbance, including blurring, light sensitivity, floaters, or blind spots; these are usually reversible but warrant stopping the drug and seeking medical evaluation, as persistent visual changes have been reported. In its approved use for ovulation induction, clomiphene increases the chance of multiple pregnancy and can cause ovarian enlargement and, less commonly, ovarian hyperstimulation syndrome. It is contraindicated in pregnancy and in people with liver disease, abnormal uterine bleeding of undetermined cause, or hormone-sensitive tumors.
Current Research Status
Clomiphene citrate is an FDA-approved prescription medication, marketed as Clomid among other names, approved for ovulation induction in women with certain types of infertility. Its use in men, including for male hypogonadism or fertility, and its use alongside anabolic steroid cycles, are off-label and not part of the approved indication. As a prescription drug it should be used under medical supervision.
Further reading: Enclomiphene, the trans-isomer of clomiphene, is reviewed in Enclomiphene: The SERM Studied for Testosterone.
Frequently Asked Questions
What is clomiphene citrate?
Clomiphene, sold as Clomid, is one of the oldest and most extensively studied selective estrogen receptor modulators (SERMs). It is an FDA-approved prescription medicine, approved in 1967, used mainly to treat infertility in women by stimulating ovulation.
How does clomiphene work?
Clomiphene competitively blocks estrogen receptors in the hypothalamus and pituitary. The brain reads this as low estrogen and increases release of gonadotropins, which stimulate the ovaries to ovulate or, in men, the testes to produce testosterone.
Is clomiphene FDA-approved?
Yes. Clomiphene is FDA-approved for ovulation induction in women with certain types of infertility. Its use in men, including for male hypogonadism or fertility, and its use alongside anabolic steroid cycles, are off-label.
What does the research say about clomiphene?
The foundational clinical study by Greenblatt and colleagues (1961) established clomiphene’s efficacy in inducing ovulation in anovulatory women. It has decades of clinical data in fertility medicine and a long-characterized safety profile.
What are the safety concerns with clomiphene?
Common adverse effects include hot flashes, mood changes, headache, breast tenderness and abdominal discomfort. A distinctive and clinically important effect is visual disturbance, including blurring and light sensitivity, which warrants stopping the drug and medical review.
Research Handling & Storage
Storage
- Unopened: Store at controlled room temperature, 20–25°C (68–77°F), away from direct sunlight, heat, and moisture.
- Opened: Keep container tightly closed. Use within the timeframe indicated on the label, typically 30–90 days after opening.
- Do not freeze liquid solutions unless specifically indicated.
Handling Precautions
- Handle with appropriate personal protective equipment (PPE) including nitrile gloves, lab coat, and eye protection.
- Use aseptic/sterile technique when reconstituting and transferring solutions to prevent contamination.
- Avoid repeated freeze-thaw cycles which may denature the compound and reduce potency.
- Keep detailed laboratory records including reconstitution dates, lot numbers, concentrations, and storage conditions.
- Dispose of unused material and sharps in accordance with local regulations and institutional biosafety guidelines.
Stability & Shelf Life
Liquid formulations typically remain stable for 1–2 years when stored at the recommended temperature in the original sealed container. Once opened, potency may gradually decrease. Monitor for any changes in color, clarity, or odor, which may indicate degradation.
Purity & Quality Considerations
Research-grade compounds should be accompanied by a Certificate of Analysis (COA) confirming purity, typically verified by High-Performance Liquid Chromatography (HPLC) and Mass Spectrometry (MS). Look for purity levels of ≥98% for research applications. Third-party testing adds an additional layer of quality assurance. Always verify the source and documentation before using any research compound.
Research Supplies & Resources
Essential supplies and educational resources for peptide research. Links go to Amazon.com.
Lab Supplies
Recommended Reading
Lab Equipment
As an Amazon Associate, peptides.fyi earns from qualifying purchases. Learn more.