Synopsis
Compound overview
- Research only
- In clinical trials
- Approved outside US
- FDA-approved
What it is
Anastrozole (Arimidex) is an aromatase inhibitor. It is an FDA-approved prescription medicine, used mainly to treat hormone-receptor-positive breast cancer in post-menopausal women.
What it does
Documented and off-label uses include:
- Treats hormone-receptor-positive breast cancer
- Lowers estrogen levels in the body
- Used off-label by some men to control estrogen
- Has extensive clinical data
How it works
Anastrozole blocks aromatase, the enzyme that converts androgens into estrogen. With less estrogen being made, estrogen-sensitive cancer cells lose the signal that drives their growth.
Safety notes
Anastrozole is a prescription cancer medicine. Lowering estrogen too far causes joint pain, hot flushes and, over time, bone-density loss. Self-directed use to "control estrogen" can push estrogen too low, which carries its own health risks. Research-vendor material is not pharmacy-grade.
Where to buy Anastrozole
Standard lyophilized vial — reconstitute and measure doses yourself. The conventional research format.
Affiliate links — we may earn a commission at no extra cost to you.
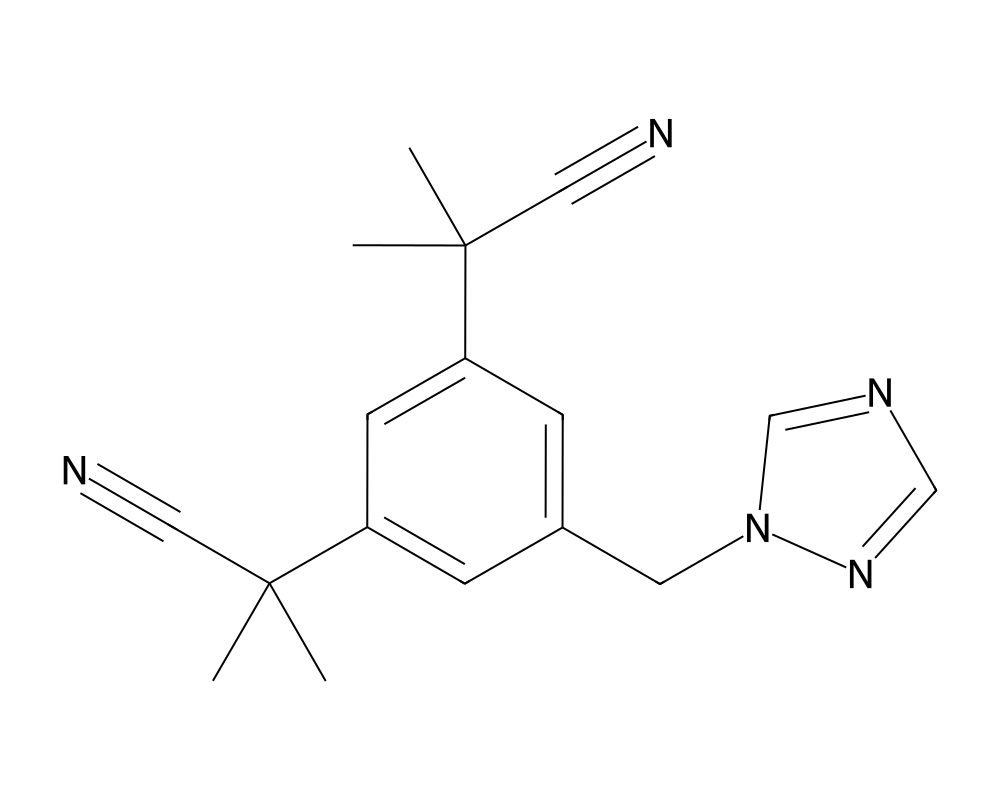
Molecular Structure
Overview
Anastrozole is a third-generation non-steroidal aromatase inhibitor developed by AstraZeneca and marketed under the brand name Arimidex. It belongs to the triazole class of compounds and acts as a potent, selective, and reversible inhibitor of the aromatase enzyme (CYP19A1). Anastrozole was first approved by the FDA in 1995 for the treatment of advanced breast cancer in postmenopausal women and has since become one of the most widely prescribed aromatase inhibitors worldwide.
Contents
- Overview
- Mechanism of Action
- Triazole-Heme Coordination
- Selectivity Profile
- Estrogen Suppression Dynamics
- Research Summary
- ATAC Trial
- Dose Optimization and Pharmacokinetics
- Bone Health Considerations
- Dosing in Published Research
- Safety and Side Effects
- Current Research Status
- Frequently Asked Questions
Unlike steroidal aromatase inhibitors such as exemestane, anastrozole does not possess structural similarity to androgens and does not form a permanent covalent bond with the enzyme. Instead, it binds competitively and reversibly to the heme group within the aromatase active site through coordination of its triazole nitrogen with the iron atom. This reversible binding means that aromatase activity can recover relatively quickly upon discontinuation of the drug, with estrogen levels typically returning to baseline within 2-3 weeks.
At the standard clinical dose of 1 mg daily, anastrozole suppresses circulating estradiol levels by approximately 80-90% in postmenopausal women. The drug has excellent oral bioavailability and a terminal elimination half-life of approximately 40-50 hours, supporting once-daily dosing. Anastrozole is primarily metabolized through N-dealkylation, hydroxylation, and glucuronidation, with the majority of the dose excreted renally.
Mechanism of Action
Anastrozole inhibits the aromatase enzyme through competitive, reversible binding to the enzyme’s active site. Aromatase catalyzes the rate-limiting step in estrogen biosynthesis: the conversion of androstenedione to estrone and testosterone to estradiol. By blocking this conversion, anastrozole effectively reduces circulating estrogen levels throughout the body.
Triazole-Heme Coordination
The mechanism of inhibition involves the coordination of the triazole nitrogen in anastrozole with the iron atom of the heme prosthetic group at the active site of CYP19A1. This coordination displaces the oxygen molecule normally bound to the heme iron, preventing the oxidative reactions necessary for aromatization of the A-ring of the androgen substrate. The two nitrile-substituted benzyl groups flanking the triazole ring provide hydrophobic interactions with residues in the substrate-binding pocket, conferring high selectivity for aromatase over other cytochrome P450 enzymes.
Selectivity Profile
Anastrozole demonstrates high selectivity for aromatase relative to other steroidogenic cytochrome P450 enzymes. At therapeutic concentrations, it does not significantly affect the biosynthesis of cortisol, aldosterone, or other adrenal steroids. This selectivity is clinically important because earlier-generation aromatase inhibitors such as aminoglutethimide lacked this selectivity and caused adrenal insufficiency requiring glucocorticoid replacement. Studies have confirmed that anastrozole at doses up to 10 mg daily does not affect basal or ACTH-stimulated cortisol or aldosterone levels.
Estrogen Suppression Dynamics
Following oral administration, anastrozole achieves steady-state plasma concentrations within approximately 7 days of daily dosing. At steady state, the drug produces approximately 80-90% suppression of plasma estradiol, estrone, and estrone sulfate. The degree of estrogen suppression is dose-dependent up to 1 mg, with minimal additional suppression at higher doses, establishing 1 mg as the optimal clinical dose.
Research Summary
Anastrozole has been evaluated in several landmark clinical trials that established aromatase inhibitors as the standard of care in hormone receptor-positive breast cancer treatment.
ATAC Trial
The Arimidex, Tamoxifen, Alone or in Combination (ATAC) trial, first reported in The Lancet (2002), was a pivotal Phase III study that randomized 9,366 postmenopausal women with early-stage hormone receptor-positive breast cancer to receive anastrozole, tamoxifen, or the combination as adjuvant therapy for 5 years. The trial demonstrated that anastrozole significantly improved disease-free survival compared to tamoxifen (HR 0.87, 95% CI 0.78-0.97, p=0.01), with a 26% reduction in contralateral breast cancer risk. Anastrozole was also associated with fewer thromboembolic events and endometrial cancers but more musculoskeletal complaints and fractures compared to tamoxifen. The combination arm showed no advantage over tamoxifen alone and was discontinued.
Dose Optimization and Pharmacokinetics
Buzdar et al. (2006) published comprehensive pharmacokinetic analyses demonstrating the dose-response relationship of anastrozole. These studies established that 1 mg daily provides near-maximal aromatase inhibition and confirmed the drug’s favorable pharmacokinetic profile, including high oral bioavailability, linear pharmacokinetics, and minimal drug-drug interactions mediated through CYP450 enzymes. The terminal elimination half-life of 40-50 hours supports steady-state maintenance with once-daily dosing.
Bone Health Considerations
Long-term follow-up of aromatase inhibitor trials has identified bone mineral density loss as a significant clinical concern. The profound estrogen suppression achieved by anastrozole accelerates bone resorption, resulting in approximately 2-4% loss of bone mineral density per year during treatment. This has led to clinical guidelines recommending baseline and periodic bone density monitoring for patients receiving aromatase inhibitor therapy, with bisphosphonate or denosumab co-administration when clinically indicated.
Dosing in Published Research
About this section
The information below reports dosing only as it appears in published clinical or preclinical research and official regulatory documents. It is provided as published-literature reference material. It is not dosing guidance, not medical advice, and not a recommendation to use or self-administer this compound.
Anastrozole is an FDA-approved prescription medicine, sold as Arimidex. According to the FDA-approved labeling, the dose across its breast-cancer indications in postmenopausal women is one 1 mg tablet taken once daily, with treatment in the advanced-disease setting continued until tumor progression. These figures are drawn from FDA-approved prescribing information.
Important
The 1 mg dose applies to the approved prescription product used under the supervision of an oncologist or physician. It is not a recommendation. Use of anastrozole outside its labeled oncology indications is off-label and is not described by this labeling.
Safety and Side Effects
Anastrozole is an FDA-approved drug with a well-characterized safety profile. Common adverse effects include hot flashes, joint and muscle pain (which can be substantial and is a frequent reason for discontinuation), fatigue, mood changes, and headache. Its most clinically significant long-term effect follows from estrogen suppression: anastrozole reduces bone mineral density and increases the risk of osteoporosis and fractures, and bone health is monitored during treatment. It can adversely affect the lipid profile, and a higher rate of ischemic cardiovascular events has been reported in some comparative data. Anastrozole is contraindicated in pregnancy because of the risk of fetal harm, and it has no role in premenopausal women without ovarian suppression.
Current Research Status
Anastrozole is an FDA-approved prescription medication, marketed as Arimidex, approved for the treatment of hormone-receptor-positive breast cancer in postmenopausal women. Use outside that setting, including off-label use to control estrogen in men using anabolic steroids, is not an approved indication and is not supported by the approval. As a prescription drug it should be used under medical supervision.
Frequently Asked Questions
What is anastrozole?
Anastrozole, brand name Arimidex, is a third-generation non-steroidal aromatase inhibitor. It is an FDA-approved prescription medicine used mainly to treat hormone-receptor-positive breast cancer in postmenopausal women.
How does anastrozole work?
Anastrozole reversibly binds and blocks the aromatase enzyme (CYP19A1), which carries out the rate-limiting step in estrogen production by converting androgens into estrogen. This substantially lowers estrogen levels.
Is anastrozole FDA-approved?
Yes. Anastrozole is FDA-approved for the treatment of hormone-receptor-positive breast cancer in postmenopausal women. Off-label use to control estrogen in men, including those using anabolic steroids, is not an approved indication.
What does the research say about anastrozole?
Anastrozole was evaluated in landmark trials, including the ATAC trial first reported in The Lancet (2002), which helped establish aromatase inhibitors as a standard of care in hormone-receptor-positive breast cancer. It has extensive clinical data.
What are the safety concerns with anastrozole?
Common adverse effects include hot flashes, joint and muscle pain (which can be substantial and is a frequent reason for discontinuation), fatigue, mood changes and headache. Its most significant long-term effect is accelerated loss of bone mineral density.
Research Handling & Storage
Storage
- Unopened: Store at controlled room temperature, 20–25°C (68–77°F), away from direct sunlight, heat, and moisture.
- Opened: Keep container tightly closed. Use within the timeframe indicated on the label, typically 30–90 days after opening.
- Do not freeze liquid solutions unless specifically indicated.
Handling Precautions
- Handle with appropriate personal protective equipment (PPE) including nitrile gloves, lab coat, and eye protection.
- Use aseptic/sterile technique when reconstituting and transferring solutions to prevent contamination.
- Avoid repeated freeze-thaw cycles which may denature the compound and reduce potency.
- Keep detailed laboratory records including reconstitution dates, lot numbers, concentrations, and storage conditions.
- Dispose of unused material and sharps in accordance with local regulations and institutional biosafety guidelines.
Stability & Shelf Life
Liquid formulations typically remain stable for 1–2 years when stored at the recommended temperature in the original sealed container. Once opened, potency may gradually decrease. Monitor for any changes in color, clarity, or odor, which may indicate degradation.
Purity & Quality Considerations
Research-grade compounds should be accompanied by a Certificate of Analysis (COA) confirming purity, typically verified by High-Performance Liquid Chromatography (HPLC) and Mass Spectrometry (MS). Look for purity levels of ≥98% for research applications. Third-party testing adds an additional layer of quality assurance. Always verify the source and documentation before using any research compound.
Research Supplies & Resources
Essential supplies and educational resources for peptide research. Links go to Amazon.com.
Lab Supplies
Recommended Reading
Lab Equipment
As an Amazon Associate, peptides.fyi earns from qualifying purchases. Learn more.