Synopsis
Compound overview
- Research only
- In clinical trials
- Approved outside US
- FDA-approved
What it is
Exemestane (Aromasin) is an aromatase inhibitor. It is an FDA-approved prescription medicine, used to treat hormone-receptor-positive breast cancer in post-menopausal women.
What it does
Documented and off-label uses include:
- Treats hormone-receptor-positive breast cancer
- Lowers estrogen levels in the body
- Used off-label by some men to control estrogen
- Has documented clinical data
How it works
Exemestane permanently disables aromatase — the enzyme that converts androgens into estrogen — which is why it is sometimes called a "suicide" inhibitor. The result is lower estrogen levels.
Safety notes
Exemestane is a prescription cancer medicine. It can cause joint pain, hot flushes, fatigue and, with long-term use, bone-density loss. Using it without medical oversight risks driving estrogen too low. Research-vendor material is not pharmacy-grade.
Where to buy Exemestane
Standard lyophilized vial — reconstitute and measure doses yourself. The conventional research format.
Affiliate links — we may earn a commission at no extra cost to you.
Molecular Structure
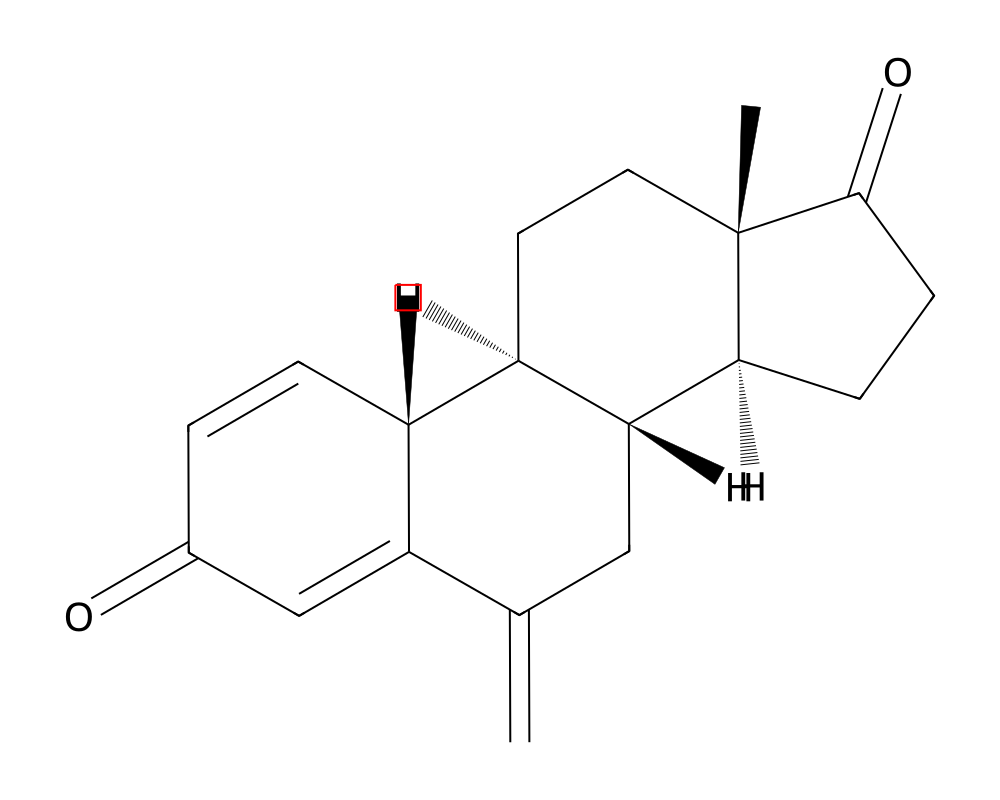
Overview
Exemestane is a third-generation steroidal aromatase inhibitor that functions as an irreversible, mechanism-based inactivator of the cytochrome P450 aromatase enzyme (CYP19A1). Unlike non-steroidal aromatase inhibitors such as anastrozole and letrozole, exemestane is structurally related to the natural substrate androstenedione and binds to the active site of aromatase in an irreversible manner, earning it the designation of a “suicide inhibitor.” Once bound, the enzyme processes exemestane into a reactive intermediate that forms a covalent bond with the enzyme, permanently inactivating it. New estrogen synthesis can only resume once the body produces fresh aromatase protein.
Contents
- Overview
- Mechanism of Action
- Suicide Inhibition Mechanism
- Androgenic Properties
- Endocrine Effects
- Research Summary
- Intergroup Exemestane Study (IES)
- Pharmacokinetic and Dose-Response Studies
- MAP.3 Breast Cancer Prevention Trial
- Dosing in Published Research
- Safety and Side Effects
- Current Research Status
- Frequently Asked Questions
Exemestane was approved by the FDA in 1999 under the brand name Aromasin, initially for the treatment of advanced breast cancer in postmenopausal women whose disease had progressed following tamoxifen therapy. Its indication was subsequently expanded to include adjuvant treatment of early-stage hormone receptor-positive breast cancer. The drug represented an important advancement in endocrine therapy by offering a mechanistically distinct alternative to the non-steroidal aromatase inhibitors and to the selective estrogen receptor modulators (SERMs) that had previously dominated breast cancer treatment.
In clinical practice, exemestane typically reduces circulating estrogen levels by 85-95% in postmenopausal women. Importantly, because exemestane is an androstane derivative, it possesses mild androgenic activity and does not adversely affect lipid profiles to the same degree as non-steroidal aromatase inhibitors, a distinction that has been noted in comparative endocrine studies.
Mechanism of Action
Exemestane exerts its pharmacological effects through irreversible inactivation of the aromatase enzyme complex. Aromatase (CYP19A1) is the sole enzyme responsible for the final step in estrogen biosynthesis, catalyzing the conversion of androgens (androstenedione and testosterone) to estrogens (estrone and estradiol, respectively). This reaction involves three sequential hydroxylation steps, each consuming one molecule of NADPH and molecular oxygen.
Suicide Inhibition Mechanism
Exemestane mimics the natural substrate androstenedione and is initially processed by aromatase through normal catalytic steps. During this processing, the enzyme converts exemestane into a chemically reactive intermediate that forms an irreversible covalent bond with the aromatase active site. Specifically, the C-1,2 double bond and the methylene group at position 6 of exemestane are critical for this mechanism-based inactivation. The resulting enzyme-inhibitor complex is catalytically dead and cannot be regenerated, meaning that estrogen production from that particular enzyme molecule is permanently halted.
Androgenic Properties
Unlike the non-steroidal aromatase inhibitors, exemestane and its primary metabolite 17-hydroexemestane possess weak androgenic activity. The 17-hydroexemestane metabolite has been shown to bind to androgen receptors with moderate affinity, which may account for certain clinical observations including relatively neutral effects on bone mineral density compared to letrozole, as well as the preservation of more favorable lipid profiles in some comparative studies. This androgenic character is a unique pharmacological feature among the approved aromatase inhibitors.
Endocrine Effects
At the standard clinical dose of 25 mg daily, exemestane suppresses plasma estradiol, estrone, and estrone sulfate by approximately 85-95% from baseline in postmenopausal women. The maximal suppression is achieved within 2-3 days of initiating therapy, and the effect persists for 4-5 days following a single dose due to the irreversible nature of enzyme inactivation. Recovery of aromatase activity after cessation of exemestane requires de novo synthesis of new enzyme protein, a process that takes approximately 2-3 weeks.
Research Summary
Exemestane has been evaluated in multiple large-scale randomized controlled trials, establishing its role as a cornerstone of endocrine therapy for hormone receptor-positive breast cancer.
Intergroup Exemestane Study (IES)
The landmark Intergroup Exemestane Study, published by Coombes et al. (2004) in the New England Journal of Medicine, enrolled 4,742 postmenopausal women with early breast cancer who had already received 2-3 years of adjuvant tamoxifen. Patients were randomized to switch to exemestane or continue tamoxifen for the remainder of a 5-year treatment period. The study demonstrated a significant improvement in disease-free survival with exemestane (HR 0.68, 95% CI 0.56-0.82, p<0.001), corresponding to a 32% reduction in the risk of recurrence. Updated long-term follow-up data confirmed the durability of these benefits.
Pharmacokinetic and Dose-Response Studies
Lonning et al. (2000) conducted detailed pharmacokinetic studies demonstrating that exemestane achieves peak plasma concentrations within 2 hours of oral administration, with an elimination half-life of approximately 24 hours. The study confirmed near-complete suppression of aromatase activity at the 25 mg daily dose and established the dose-response relationship for estrogen suppression. The oral bioavailability increases by approximately 40% when taken with a high-fat meal, informing the clinical recommendation to administer exemestane after food.
MAP.3 Breast Cancer Prevention Trial
The NCIC CTG MAP.3 trial evaluated exemestane for breast cancer risk reduction in high-risk postmenopausal women. Goss et al. (2011) published results in the New England Journal of Medicine showing a 65% relative reduction in invasive breast cancer incidence with exemestane versus placebo over a median follow-up of 35 months, providing evidence for the drug’s chemopreventive potential.
Dosing in Published Research
About this section
The information below reports dosing only as it appears in published clinical or preclinical research and official regulatory documents. It is provided as published-literature reference material. It is not dosing guidance, not medical advice, and not a recommendation to use or self-administer this compound.
Exemestane is an FDA-approved prescription medicine, sold as Aromasin. According to the FDA-approved labeling, the dose is one 25 mg tablet taken once daily after a meal, with treatment in the advanced-disease setting continued until tumor progression. These figures are drawn from FDA-approved prescribing information.
Important
The 25 mg dose applies to the approved prescription product used under the supervision of an oncologist or physician. It is not a recommendation, and use outside the labeled oncology indications is off-label and is not described by this labeling.
Safety and Side Effects
Exemestane is an FDA-approved drug with a well-characterized safety profile. Common adverse effects include hot flashes, fatigue, joint and muscle pain, and headache. Clinically important is its effect on bone: by suppressing estrogen, exemestane accelerates the loss of bone mineral density and increases the risk of osteoporosis and fracture, so bone health is monitored during treatment. It can also affect lipid levels. Exemestane is contraindicated in pregnancy and in premenopausal women without appropriate ovarian suppression, because of the risk of harm to a fetus and because estrogen suppression behaves differently in premenopausal physiology.
Current Research Status
Exemestane is an FDA-approved prescription medication, marketed as Aromasin, approved for the treatment of estrogen-receptor-positive breast cancer in postmenopausal women, including in the adjuvant setting and after tamoxifen. Use outside oncology, including off-label use as an estrogen-control agent alongside anabolic steroids, is not an approved indication and is not supported by the approval. As a prescription drug it should be used under medical supervision.
Frequently Asked Questions
What is exemestane?
Exemestane, brand name Aromasin, is a third-generation steroidal aromatase inhibitor. It is an FDA-approved prescription medicine used to treat hormone-receptor-positive breast cancer in postmenopausal women.
How does exemestane work?
Exemestane is a mechanism-based inactivator: it permanently disables the aromatase enzyme (CYP19A1), which carries out the final step in estrogen production. Because the inactivation is irreversible, estrogen levels remain suppressed until new enzyme is made.
Is exemestane FDA-approved?
Yes. Exemestane is FDA-approved for estrogen-receptor-positive breast cancer in postmenopausal women, including in the adjuvant setting and after tamoxifen. Off-label use as an estrogen-control agent is not an approved indication.
What does the research say about exemestane?
Exemestane has been evaluated in large randomized controlled trials, including the Intergroup Exemestane Study reported by Coombes and colleagues (2004), which supported its role in endocrine therapy for hormone-receptor-positive breast cancer.
What are the safety concerns with exemestane?
Common adverse effects include hot flashes, fatigue, joint and muscle pain and headache. A clinically important effect is on bone: by suppressing estrogen, exemestane accelerates loss of bone mineral density and increases fracture risk.
Research Handling & Storage
Storage
- Unopened: Store at controlled room temperature, 20–25°C (68–77°F), away from direct sunlight, heat, and moisture.
- Opened: Keep container tightly closed. Use within the timeframe indicated on the label, typically 30–90 days after opening.
- Do not freeze liquid solutions unless specifically indicated.
Handling Precautions
- Handle with appropriate personal protective equipment (PPE) including nitrile gloves, lab coat, and eye protection.
- Use aseptic/sterile technique when reconstituting and transferring solutions to prevent contamination.
- Avoid repeated freeze-thaw cycles which may denature the compound and reduce potency.
- Keep detailed laboratory records including reconstitution dates, lot numbers, concentrations, and storage conditions.
- Dispose of unused material and sharps in accordance with local regulations and institutional biosafety guidelines.
Stability & Shelf Life
Liquid formulations typically remain stable for 1–2 years when stored at the recommended temperature in the original sealed container. Once opened, potency may gradually decrease. Monitor for any changes in color, clarity, or odor, which may indicate degradation.
Purity & Quality Considerations
Research-grade compounds should be accompanied by a Certificate of Analysis (COA) confirming purity, typically verified by High-Performance Liquid Chromatography (HPLC) and Mass Spectrometry (MS). Look for purity levels of ≥98% for research applications. Third-party testing adds an additional layer of quality assurance. Always verify the source and documentation before using any research compound.
Research Supplies & Resources
Essential supplies and educational resources for peptide research. Links go to Amazon.com.
Lab Supplies
Recommended Reading
Lab Equipment
As an Amazon Associate, peptides.fyi earns from qualifying purchases. Learn more.