Synopsis
Compound overview
- Research only
- In clinical trials
- Approved outside US
- FDA-approved
What it is
Letrozole (Femara) is an aromatase inhibitor. It is an FDA-approved prescription medicine, used mainly to treat hormone-receptor-positive breast cancer and, in some cases, to help with ovulation.
What it does
Documented and off-label uses include:
- Treats hormone-receptor-positive breast cancer
- Strongly lowers estrogen levels
- Also used to induce ovulation in fertility care
- Used off-label by some men to control estrogen
How it works
Letrozole blocks aromatase, the enzyme that turns androgens into estrogen, sharply reducing how much estrogen the body produces.
Safety notes
Letrozole is a prescription medicine and a potent estrogen-lowering drug. Side effects include joint and bone pain, hot flushes and bone-density loss, and pushing estrogen too low brings its own risks. It should be used under medical supervision; research-vendor material is not pharmacy-grade.
Where to buy Letrozole
Standard lyophilized vial — reconstitute and measure doses yourself. The conventional research format.
Affiliate links — we may earn a commission at no extra cost to you.
Molecular Structure
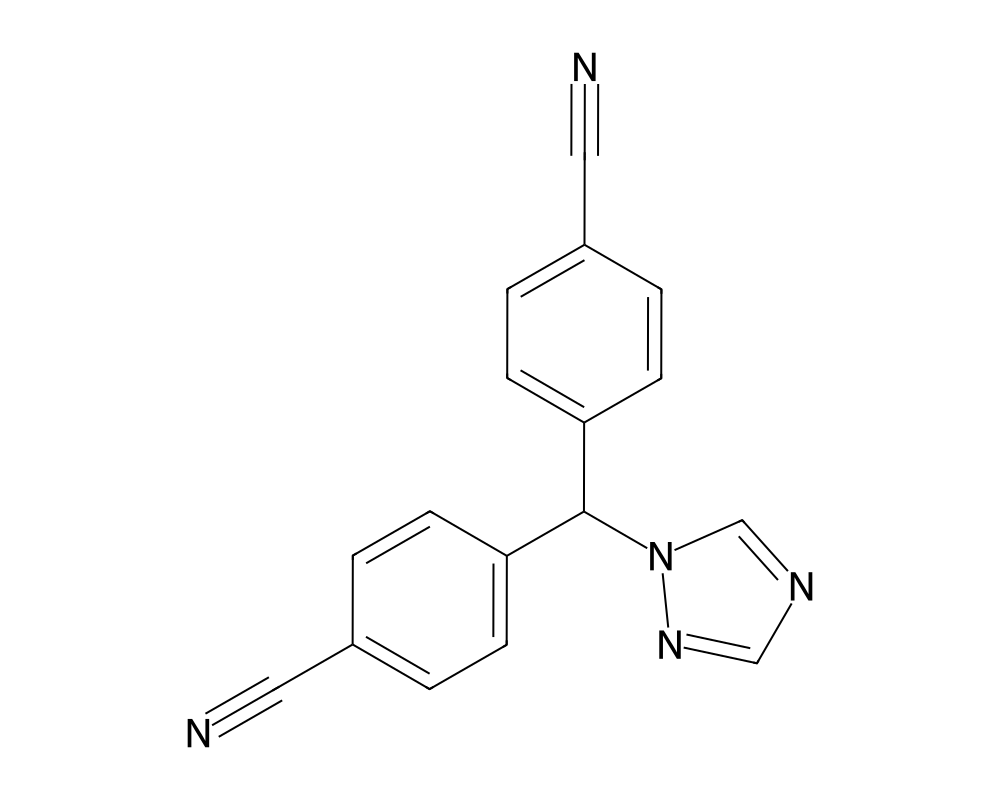
Overview
Letrozole is a third-generation non-steroidal aromatase inhibitor originally developed by Novartis and marketed under the brand name Femara. It received FDA approval in 1997 for the treatment of hormone receptor-positive breast cancer in postmenopausal women. Since then, it has become one of the most widely prescribed aromatase inhibitors in oncology, used in both adjuvant and metastatic settings. The compound has also gained significant off-label traction in fertility medicine and, within the research community, as a tool for investigating estrogen-dependent physiological processes.
Contents
Aromatase, the enzyme letrozole targets, catalyzes the final step in estrogen biosynthesis: the conversion of androgens (testosterone and androstenedione) into estrogens (estradiol and estrone). By inhibiting this enzyme, letrozole has been shown to suppress circulating estrogen levels by more than 95% in postmenopausal women in published studies. This degree of estrogen suppression is unmatched by first- and second-generation aromatase inhibitors, which is why letrozole and its third-generation counterparts have largely replaced them in clinical practice.
Mechanism of Action
Letrozole binds reversibly to the heme group of the cytochrome P450 aromatase enzyme (CYP19A1), occupying the substrate-binding site and preventing androgen substrates from accessing the catalytic center. This competitive inhibition is highly selective; letrozole shows minimal activity against other cytochrome P450 enzymes at therapeutic concentrations, which limits off-target hormonal disruption.
The pharmacological consequence is a dramatic reduction in estrogen synthesis across all tissue compartments where aromatase is expressed, including adipose tissue, bone, brain, and (in premenopausal women) the ovaries. In postmenopausal women, where ovarian estrogen production has ceased and peripheral aromatization in fat and other tissues is the primary estrogen source, letrozole effectively eliminates nearly all circulating estrogen.
In premenopausal women and in males, the estrogen suppression triggers a distinct feedback response. The hypothalamus senses falling estradiol levels and increases GnRH pulsatility, driving up LH and FSH secretion. In women, this mechanism underlies letrozole’s effectiveness as an ovulation induction agent. In men, the resulting LH elevation stimulates testicular testosterone production, which is why researchers have investigated the compound in the context of male hypogonadism and HPG axis manipulation.
Research Summary
In oncology, letrozole’s evidence base is formidable. The BIG 1-98 trial, involving over 8,000 postmenopausal women with hormone receptor-positive early breast cancer, demonstrated that letrozole significantly improved disease-free survival compared to tamoxifen when used as initial adjuvant therapy. Extended adjuvant studies, including MA.17 and its follow-up MA.17R, showed that letrozole continued to reduce recurrence risk even when initiated after five years of tamoxifen therapy.
In reproductive medicine, letrozole has emerged as a first-line ovulation induction agent for women with polycystic ovary syndrome (PCOS). The landmark NICHD trial published in the New England Journal of Medicine in 2014 demonstrated superior live birth rates with letrozole compared to clomiphene citrate in this population, with lower rates of multiple gestations. This study fundamentally shifted clinical practice in reproductive endocrinology.
Research in male subjects has explored letrozole’s ability to increase the testosterone-to-estradiol ratio. Studies in adolescent males with idiopathic short stature showed that aromatase inhibition could delay epiphyseal fusion and increase predicted adult height. In adult men with obesity-related hypogonadism, where excessive aromatization of testosterone to estradiol contributes to HPG axis suppression, letrozole has shown the ability to normalize testosterone levels.
Pharmacokinetic studies reveal a terminal half-life of approximately 48 hours, supporting once-daily dosing. The compound is metabolized primarily by CYP3A4 and CYP2A6, with renal excretion of metabolites. Steady-state plasma concentrations are reached within two to six weeks of daily administration.
Dosing in Published Research
About this section
The information below reports dosing only as it appears in published clinical or preclinical research and official regulatory documents. It is provided as published-literature reference material. It is not dosing guidance, not medical advice, and not a recommendation to use or self-administer this compound.
Letrozole is an FDA-approved prescription medicine, sold as Femara. According to the FDA-approved labeling, the dose across its breast-cancer indications in postmenopausal women is one 2.5 mg tablet taken once daily, with or without food, and treatment in the advanced-disease setting continued until tumor progression. These figures are drawn from FDA-approved prescribing information.
Important
The 2.5 mg dose applies to the approved prescription product used under the supervision of an oncologist or physician. It is not a recommendation. Other uses of letrozole, such as ovulation induction, are off-label and are not described by this labeling.
Safety and Side Effects
The side effect profile of letrozole reflects the consequences of profound estrogen depletion. In postmenopausal women undergoing long-term treatment, the most clinically significant adverse effects include accelerated bone mineral density loss and increased fracture risk. Musculoskeletal symptoms, including arthralgia and myalgia, affect a substantial proportion of patients and represent the most common reason for treatment discontinuation in the adjuvant setting.
Hot flashes, fatigue, and headache are frequently reported. Lipid profile changes, including modest elevations in total and LDL cholesterol, have been observed in some studies, though the cardiovascular significance of these changes remains debated. Hepatic transaminase elevations occur rarely and are typically reversible upon discontinuation.
In male subjects, the primary concern with aromatase inhibitor use is excessive estrogen suppression. Estradiol plays important roles in male bone health, cardiovascular function, sexual function, and mood. Over-suppression can produce symptoms including joint pain, decreased libido, erectile dysfunction, and adverse lipid changes. Careful dose titration and monitoring of estradiol levels are considered essential in research protocols involving male subjects.
Teratogenicity is a significant concern. Letrozole is classified as Pregnancy Category X, and strict contraceptive measures are required during and after treatment in women of reproductive potential.
Current Research Status
Letrozole is an FDA-approved medication with robust clinical evidence across oncology and reproductive medicine. Ongoing research is exploring its role in breast cancer prevention, optimal duration of adjuvant therapy, and potential applications in endometriosis management. In male health research, investigators continue to study letrozole as an alternative to testosterone replacement therapy, particularly in men with functional hypogonadism related to obesity or metabolic syndrome. The compound remains one of the most pharmacologically potent and clinically versatile aromatase inhibitors available.
Frequently Asked Questions
What is letrozole?
Letrozole, brand name Femara, is a third-generation aromatase inhibitor. It is an FDA-approved prescription medicine, approved in 1997, used mainly to treat hormone-receptor-positive breast cancer and, in some cases, to induce ovulation.
How does letrozole work?
Letrozole binds reversibly to the aromatase enzyme (CYP19A1), which converts androgens into estrogen, and blocks that conversion. The result is a strong reduction in estrogen levels.
Is letrozole FDA-approved?
Yes. Letrozole is FDA-approved with a robust evidence base across oncology and reproductive medicine. Some uses, such as ovulation induction and estrogen control in men, are off-label.
What does the research say about letrozole?
In oncology its evidence base is substantial: the BIG 1-98 trial in over 8,000 postmenopausal women showed letrozole improved disease-free survival compared with tamoxifen as initial adjuvant therapy. It is also studied in fertility care for ovulation induction.
What are the safety concerns with letrozole?
The side effects reflect profound estrogen depletion. In long-term use the most clinically significant effects include accelerated bone mineral density loss and increased fracture risk, along with musculoskeletal symptoms such as joint pain.
Research Handling & Storage
Storage
- Unopened: Store at controlled room temperature, 20–25°C (68–77°F), away from direct sunlight, heat, and moisture.
- Opened: Keep container tightly closed. Use within the timeframe indicated on the label, typically 30–90 days after opening.
- Do not freeze liquid solutions unless specifically indicated.
Handling Precautions
- Handle with appropriate personal protective equipment (PPE) including nitrile gloves, lab coat, and eye protection.
- Use aseptic/sterile technique when reconstituting and transferring solutions to prevent contamination.
- Avoid repeated freeze-thaw cycles which may denature the compound and reduce potency.
- Keep detailed laboratory records including reconstitution dates, lot numbers, concentrations, and storage conditions.
- Dispose of unused material and sharps in accordance with local regulations and institutional biosafety guidelines.
Stability & Shelf Life
Liquid formulations typically remain stable for 1–2 years when stored at the recommended temperature in the original sealed container. Once opened, potency may gradually decrease. Monitor for any changes in color, clarity, or odor, which may indicate degradation.
Purity & Quality Considerations
Research-grade compounds should be accompanied by a Certificate of Analysis (COA) confirming purity, typically verified by High-Performance Liquid Chromatography (HPLC) and Mass Spectrometry (MS). Look for purity levels of ≥98% for research applications. Third-party testing adds an additional layer of quality assurance. Always verify the source and documentation before using any research compound.
Research Supplies & Resources
Essential supplies and educational resources for peptide research. Links go to Amazon.com.
Lab Supplies
Recommended Reading
Lab Equipment
As an Amazon Associate, peptides.fyi earns from qualifying purchases. Learn more.