Synopsis
Compound overview
- Research only
- In clinical trials
- Approved outside US
- FDA-approved
What it is
Tamoxifen is a selective estrogen receptor modulator (SERM). It is a long-established FDA-approved prescription medicine, used mainly to treat and prevent certain types of breast cancer.
What it does
Documented and off-label uses include:
- Treats and helps prevent hormone-receptor-positive breast cancer
- Blocks estrogen's effect in breast tissue
- Used off the research scene by some to counter estrogen side effects
- Has decades of clinical data
How it works
Tamoxifen blocks estrogen receptors in breast tissue, denying estrogen-sensitive cancer cells the hormone signal they depend on. In some other tissues it can act more like estrogen.
Safety notes
Tamoxifen is a prescription cancer medicine used under medical supervision. It carries real risks, including blood clots and a small increased risk of uterine cancer. It is not a casual supplement; research-vendor material is not pharmacy-grade and using it without medical oversight is hazardous.
Where to buy Tamoxifen
Standard lyophilized vial — reconstitute and measure doses yourself. The conventional research format.
Affiliate links — we may earn a commission at no extra cost to you.
Molecular Structure
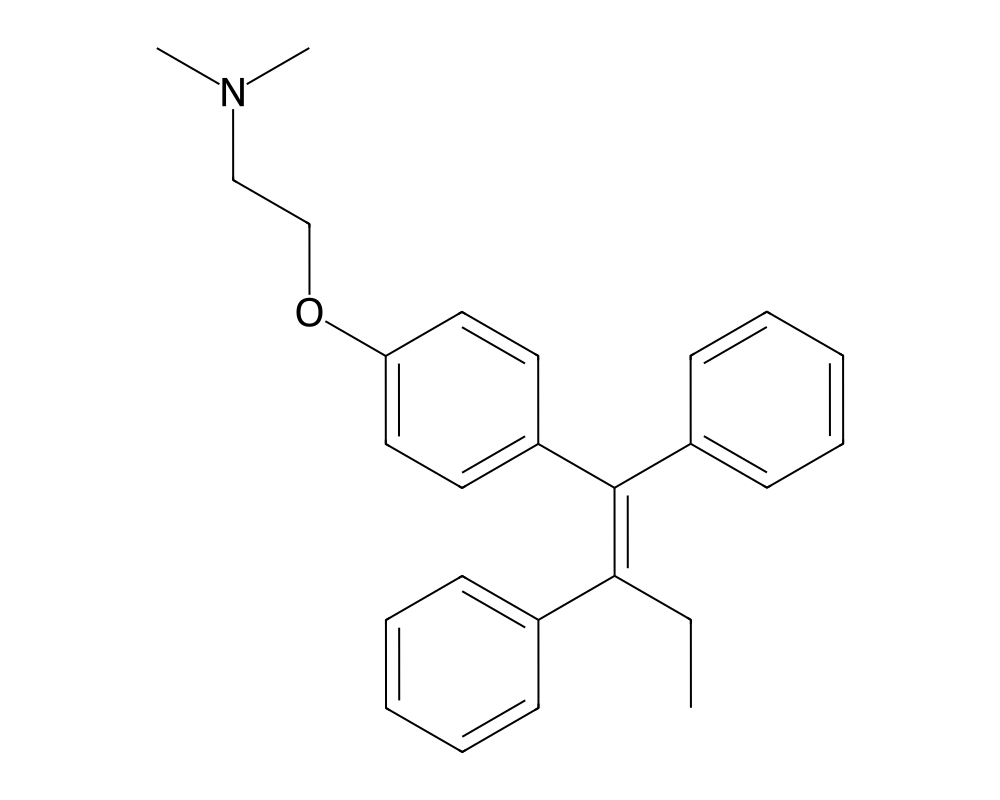
Overview
Tamoxifen is the prototypical selective estrogen receptor modulator (SERM) and one of the most extensively studied compounds in oncology. First synthesized by Dora Richardson at ICI Pharmaceuticals (now AstraZeneca) in 1962, it was originally investigated as a potential contraceptive agent before its anti-estrogenic properties in breast tissue were recognized. Tamoxifen received FDA approval for metastatic breast cancer in 1977 and for adjuvant therapy in 1986, and it has since been estimated to have been associated with substantial improvements in breast cancer survival in published studies.
Contents
- Overview
- Mechanism of Action
- Anti-Estrogenic Activity in Breast Tissue
- CYP2D6-Dependent Bioactivation
- Partial Agonist Activity
- Research Summary
- EBCTCG Meta-Analysis (2005)
- NSABP P-1 Prevention Trial
- Extended Adjuvant Therapy
- Dosing in Published Research
- Safety and Side Effects
- Current Research Status
- Frequently Asked Questions
Tamoxifen belongs to the triphenylethylene class of compounds and functions as a mixed estrogen agonist-antagonist with tissue-dependent activity. It acts as an estrogen antagonist in breast tissue, blocking estrogen-driven proliferation of hormone receptor-positive breast cancer cells, while simultaneously functioning as a partial estrogen agonist in bone, the uterus, and the cardiovascular system. This tissue-selective pharmacology was initially puzzling but is now well understood through the coregulator hypothesis of SERM action.
The drug remains on the World Health Organization’s List of Essential Medicines and continues to be used worldwide, particularly in premenopausal women with hormone receptor-positive breast cancer, for whom aromatase inhibitors are not appropriate as monotherapy. Tamoxifen is also approved for breast cancer risk reduction in high-risk women and for the treatment of ductal carcinoma in situ (DCIS).
Mechanism of Action
Tamoxifen and its active metabolites compete with estradiol for binding to estrogen receptors (ER-alpha and ER-beta). The pharmacological activity of tamoxifen is largely mediated through its primary active metabolite, endoxifen (4-hydroxy-N-desmethyltamoxifen), which has approximately 100-fold greater affinity for the estrogen receptor than the parent compound and achieves plasma concentrations sufficient for ER blockade.
Anti-Estrogenic Activity in Breast Tissue
When tamoxifen (or endoxifen) binds to ERa in breast cancer cells, it induces a conformational change in helix 12 of the ligand-binding domain that prevents the receptor from efficiently recruiting coactivator proteins essential for transcriptional activation of estrogen-responsive genes. Specifically, the aminoethoxy side chain of tamoxifen protrudes from the ligand-binding pocket and physically occludes the coactivator-binding groove (AF-2 surface). This results in suppression of estrogen-dependent cell proliferation, cell cycle arrest in G1 phase, and in some contexts, induction of apoptosis.
CYP2D6-Dependent Bioactivation
Tamoxifen is a prodrug that requires metabolic activation primarily by the cytochrome P450 enzyme CYP2D6 to generate its most potent metabolite, endoxifen. Individuals who are CYP2D6 poor metabolizers (approximately 7-10% of Caucasians) produce significantly lower endoxifen concentrations and may experience reduced clinical benefit. This pharmacogenomic relationship has been extensively debated, and while some studies have shown associations between CYP2D6 genotype and clinical outcomes, current clinical guidelines do not universally mandate CYP2D6 testing prior to tamoxifen initiation.
Partial Agonist Activity
In bone and the uterus, the tamoxifen-ER complex can recruit sufficient coactivator proteins to drive partial transcriptional activation. In bone, this estrogenic activity helps preserve bone mineral density in postmenopausal women. In the uterus, however, this agonist activity can stimulate endometrial proliferation and is associated with a 2-7-fold increased risk of endometrial cancer with long-term use, one of the most clinically significant adverse effects of tamoxifen therapy.
Research Summary
EBCTCG Meta-Analysis (2005)
The Early Breast Cancer Trialists’ Collaborative Group (EBCTCG) published a landmark meta-analysis in The Lancet (2005) encompassing data from approximately 80,000 women across 60 randomized trials. The analysis demonstrated that 5 years of adjuvant tamoxifen in women with ER-positive early breast cancer reduced the annual breast cancer death rate by 31%, with absolute 15-year survival improvements of approximately 9-10% in node-positive disease and 5-6% in node-negative disease. The benefits extended well beyond the treatment period, with continued risk reduction for at least 10 years after stopping tamoxifen.
NSABP P-1 Prevention Trial
Fisher et al. (1998) reported results from the National Surgical Adjuvant Breast and Bowel Project Prevention Trial (NSABP P-1) in the Journal of the National Cancer Institute. This landmark chemoprevention trial randomized 13,388 high-risk women to tamoxifen 20 mg daily or placebo for 5 years. Tamoxifen reduced the risk of invasive breast cancer by 49% (RR 0.51, 95% CI 0.39-0.66) and the risk of non-invasive breast cancer by 50%. This trial led to FDA approval of tamoxifen for breast cancer risk reduction in 1998.
Extended Adjuvant Therapy
The ATLAS (Adjuvant Tamoxifen: Longer Against Shorter) trial, published by Davies et al. (2013) in The Lancet, demonstrated that extending tamoxifen therapy from 5 to 10 years further reduced breast cancer recurrence and mortality. The recurrence rate reduction from years 5-14 was approximately one-third, supporting the current practice of considering extended adjuvant endocrine therapy in appropriate patients.
Dosing in Published Research
About this section
The information below reports dosing only as it appears in published clinical or preclinical research and official regulatory documents. It is provided as published-literature reference material. It is not dosing guidance, not medical advice, and not a recommendation to use or self-administer this compound.
Tamoxifen is an FDA-approved prescription medicine. The FDA-approved labeling (Nolvadex and equivalents) specifies:
- Adjuvant treatment and risk reduction of breast cancer, and ductal carcinoma in situ: 20 mg daily. The labeling notes no added benefit from doses above 20 mg per day.
- Metastatic breast cancer: 20 to 40 mg daily, with doses above 20 mg given in divided doses.
In the breast-cancer setting, treatment courses typically run 5 to 10 years. These figures are drawn from FDA-approved prescribing information.
Important
Tamoxifen carries an FDA Boxed Warning for serious and life-threatening events, including uterine malignancies, stroke, and blood clots. The labeled dose applies to the approved prescription product prescribed and monitored by a physician; it is not a recommendation and does not apply to material sold for research use.
Safety and Side Effects
Tamoxifen is an FDA-approved drug, and it carries an FDA boxed warning, the agency’s most serious warning category. The boxed warning describes serious and potentially life-threatening events that have occurred in women using tamoxifen to reduce breast cancer risk or to treat ductal carcinoma in situ: uterine malignancies, including endometrial cancer and uterine sarcoma, as well as stroke and pulmonary embolism. For women being treated for established breast cancer the benefit is generally considered to outweigh these risks, but the risks are real and require informed discussion. Common adverse effects include hot flashes, vaginal discharge or bleeding, menstrual irregularity, and mood changes. Tamoxifen increases the risk of venous thromboembolism and has been associated with cataracts and other eye changes. Any abnormal vaginal bleeding warrants prompt gynecological evaluation. It is contraindicated in pregnancy.
Current Research Status
Tamoxifen is an FDA-approved prescription medication, approved for the treatment of hormone-receptor-positive breast cancer, for ductal carcinoma in situ, and for the reduction of breast cancer risk in high-risk women. Use outside oncology, including off-label use to manage estrogenic effects during anabolic steroid use, is not an approved indication. As a prescription drug with a boxed warning, it should be used only under medical supervision.
Further reading: For a related selective estrogen receptor modulator studied in the context of testosterone, see Enclomiphene: The SERM Studied for Testosterone.
Frequently Asked Questions
What is tamoxifen?
Tamoxifen is the prototypical selective estrogen receptor modulator (SERM) and one of the most extensively studied compounds in oncology. It is a long-established FDA-approved prescription medicine used mainly to treat and prevent certain hormone-receptor-positive breast cancers.
How does tamoxifen work?
Tamoxifen and its active metabolites, chiefly endoxifen, compete with estrogen for binding at estrogen receptors. In breast tissue this blocks estrogen’s growth-promoting effect on hormone-receptor-positive cancer cells.
Is tamoxifen FDA-approved?
Yes. Tamoxifen is FDA-approved for treating hormone-receptor-positive breast cancer, for ductal carcinoma in situ and for reducing breast cancer risk in high-risk women. Use outside oncology, such as to manage estrogenic effects, is off-label.
What does the research say about tamoxifen?
A landmark 2005 meta-analysis by the Early Breast Cancer Trialists’ Collaborative Group, covering roughly 80,000 women across 60 randomized trials, found that five years of adjuvant tamoxifen substantially reduced recurrence and mortality in hormone-receptor-positive breast cancer.
What are the safety concerns with tamoxifen?
Tamoxifen carries an FDA boxed warning, the agency’s most serious warning category, describing serious and potentially life-threatening events, including uterine cancers and blood clots, observed in women using it to reduce breast cancer risk or treat ductal carcinoma in situ.
Research Handling & Storage
Storage
- Unopened: Store at controlled room temperature, 20–25°C (68–77°F), away from direct sunlight, heat, and moisture.
- Opened: Keep container tightly closed. Use within the timeframe indicated on the label, typically 30–90 days after opening.
- Do not freeze liquid solutions unless specifically indicated.
Handling Precautions
- Handle with appropriate personal protective equipment (PPE) including nitrile gloves, lab coat, and eye protection.
- Use aseptic/sterile technique when reconstituting and transferring solutions to prevent contamination.
- Avoid repeated freeze-thaw cycles which may denature the compound and reduce potency.
- Keep detailed laboratory records including reconstitution dates, lot numbers, concentrations, and storage conditions.
- Dispose of unused material and sharps in accordance with local regulations and institutional biosafety guidelines.
Stability & Shelf Life
Liquid formulations typically remain stable for 1–2 years when stored at the recommended temperature in the original sealed container. Once opened, potency may gradually decrease. Monitor for any changes in color, clarity, or odor, which may indicate degradation.
Purity & Quality Considerations
Research-grade compounds should be accompanied by a Certificate of Analysis (COA) confirming purity, typically verified by High-Performance Liquid Chromatography (HPLC) and Mass Spectrometry (MS). Look for purity levels of ≥98% for research applications. Third-party testing adds an additional layer of quality assurance. Always verify the source and documentation before using any research compound.
Research Supplies & Resources
Essential supplies and educational resources for peptide research. Links go to Amazon.com.
Lab Supplies
Recommended Reading
Lab Equipment
As an Amazon Associate, peptides.fyi earns from qualifying purchases. Learn more.