Synopsis
Compound overview
- Research only
- In clinical trials
- Approved outside US
- FDA-approved
What it is
Raloxifene (Evista) is a selective estrogen receptor modulator (SERM). It is an FDA-approved prescription medicine, used to treat and prevent osteoporosis after menopause and to reduce breast-cancer risk in some women.
What it does
Documented uses include:
- Treats and prevents osteoporosis after menopause
- Reduces breast-cancer risk in higher-risk women
- Acts like estrogen in bone but blocks it in breast tissue
- Has long-term clinical data
How it works
Raloxifene is "selective" — it activates estrogen receptors in bone, helping preserve bone density, while blocking estrogen receptors in breast tissue.
Safety notes
Raloxifene is prescription-only. It carries a known risk of blood clots and a warning about stroke risk in some women, and it can cause hot flushes and leg cramps. It should be used under medical supervision; research-vendor material is not pharmacy-grade.
Where to buy Raloxifene
Standard lyophilized vial — reconstitute and measure doses yourself. The conventional research format.
Affiliate links — we may earn a commission at no extra cost to you.
Molecular Structure
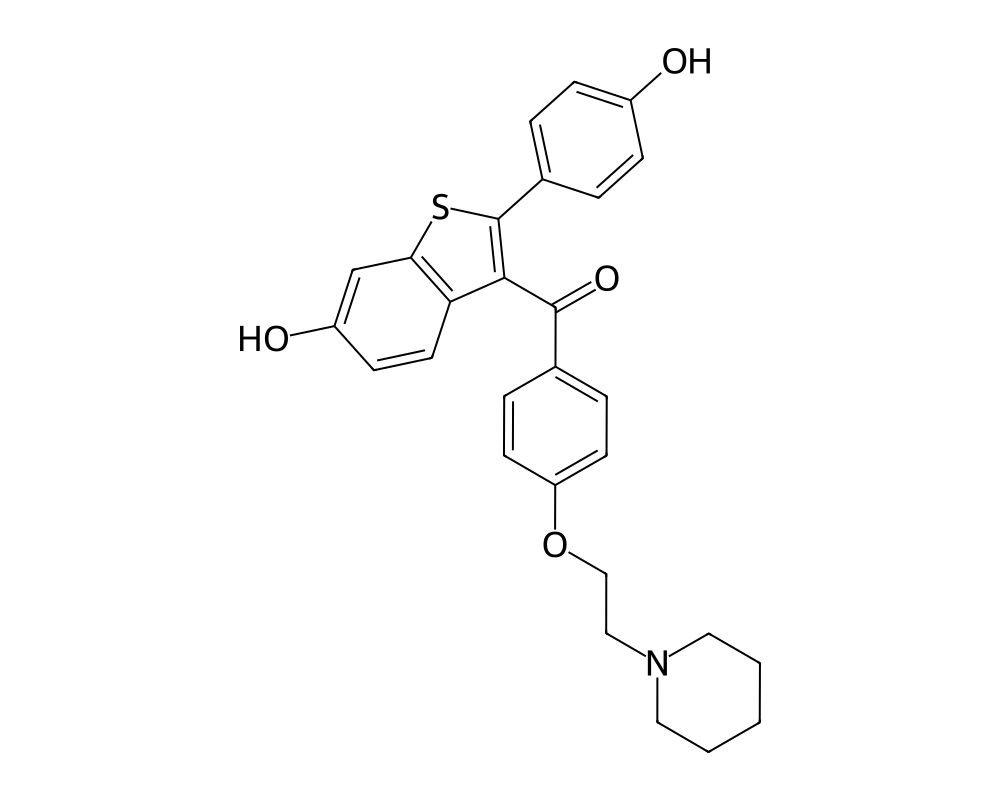
Overview
Raloxifene is a second-generation selective estrogen receptor modulator (SERM) belonging to the benzothiophene chemical class. Developed by Eli Lilly and marketed under the brand name Evista, it was first approved by the FDA in 1997 for the prevention and treatment of postmenopausal osteoporosis. In 2007, it received an additional indication for the reduction of invasive breast cancer risk in postmenopausal women with osteoporosis or at high risk for breast cancer.
Contents
- Overview
- Mechanism of Action
- Structural Basis of Tissue Selectivity
- Bone Effects
- Breast Tissue Effects
- Research Summary
- MORE Trial (Multiple Outcomes of Raloxifene Evaluation)
- Cummings et al. (1999) – Breast Cancer Risk Reduction
- STAR Trial (Study of Tamoxifen and Raloxifene)
- Dosing in Published Research
- Safety and Side Effects
- Current Research Status
- Frequently Asked Questions
Raloxifene represents a significant advancement in SERM pharmacology because it demonstrates tissue-selective estrogenic and anti-estrogenic activity with a more favorable side effect profile than tamoxifen in certain respects. In bone tissue, raloxifene acts as an estrogen agonist, preserving bone mineral density and reducing fracture risk. In breast and uterine tissue, it acts as an estrogen antagonist, reducing breast cancer incidence without stimulating endometrial proliferation. This tissue selectivity arises from the differential recruitment of coactivator and corepressor proteins to the estrogen receptor complex in different cell types.
The development of raloxifene was informed by the observation that the ideal SERM would preserve the beneficial skeletal and cardiovascular effects of estrogen while antagonizing its proliferative effects in breast and uterine tissue. While raloxifene has achieved the first two objectives, its cardiovascular effects have proven more complex, as demonstrated by the results of the RUTH (Raloxifene Use for The Heart) trial.
Mechanism of Action
Raloxifene binds to both estrogen receptor alpha (ERa) and estrogen receptor beta (ERb) with high affinity. However, unlike estradiol, raloxifene induces a distinct conformational change in the ligand-binding domain of the receptor that alters the recruitment of transcriptional coregulatory proteins in a tissue-specific manner.
Structural Basis of Tissue Selectivity
X-ray crystallographic studies have revealed that when raloxifene binds to ERa, the position of helix 12 in the ligand-binding domain differs from its position when estradiol occupies the receptor. Specifically, the bulky side chain of raloxifene sterically prevents helix 12 from adopting the agonist conformation necessary for efficient recruitment of coactivator proteins containing LXXLL motifs (such as SRC-1, SRC-2, and SRC-3). Instead, the receptor adopts a conformation that favors recruitment of corepressor proteins (NCoR, SMRT) in tissues where these corepressors are abundant, while still permitting partial agonist activity in tissues where certain coactivators predominate.
Bone Effects
In osteoblasts and osteoclasts, raloxifene functions as a partial estrogen agonist, inhibiting bone resorption through suppression of osteoclast differentiation and activity. This effect is mediated through regulation of cytokines involved in osteoclastogenesis, including RANKL, osteoprotegerin (OPG), and interleukin-6. Raloxifene increases the OPG/RANKL ratio, shifting the balance away from bone resorption and toward preservation of bone mass.
Breast Tissue Effects
In breast epithelial cells, raloxifene acts as a pure estrogen antagonist, blocking estrogen-driven proliferation and inhibiting the expression of estrogen-responsive genes involved in cell cycle progression. This anti-estrogenic activity in breast tissue underlies its efficacy in reducing invasive breast cancer incidence, particularly for estrogen receptor-positive tumors.
Research Summary
MORE Trial (Multiple Outcomes of Raloxifene Evaluation)
The MORE trial (1999), published in JAMA, was a pivotal multicenter, randomized, double-blind, placebo-controlled trial that enrolled 7,705 postmenopausal women with osteoporosis. Over 3 years, raloxifene 60 mg daily reduced the risk of vertebral fractures by 30% (RR 0.70, 95% CI 0.56-0.86) and the risk of invasive breast cancer by 72% (RR 0.28, 95% CI 0.17-0.46). This unexpected finding of breast cancer risk reduction became a primary driver of subsequent research into raloxifene’s chemopreventive potential.
Cummings et al. (1999) – Breast Cancer Risk Reduction
Cummings et al. (1999), reporting secondary endpoints from the MORE trial in JAMA, provided the first robust evidence that raloxifene significantly reduced the incidence of estrogen receptor-positive invasive breast cancer by 90% (RR 0.10, 95% CI 0.04-0.24) compared to placebo. This dramatic reduction was specific to ER-positive tumors, with no significant effect on ER-negative breast cancer, consistent with raloxifene’s mechanism as an estrogen receptor antagonist in breast tissue.
STAR Trial (Study of Tamoxifen and Raloxifene)
The NSABP STAR trial (P-2), reported by Vogel et al. (2006) in JAMA, directly compared raloxifene to tamoxifen for breast cancer risk reduction in 19,747 high-risk postmenopausal women. Raloxifene was shown to be as effective as tamoxifen in reducing invasive breast cancer risk (RR 1.02, 95% CI 0.82-1.28) while demonstrating significantly fewer thromboembolic events and cataracts, and critically, no increase in endometrial cancer risk (a known concern with tamoxifen).
Dosing in Published Research
About this section
The information below reports dosing only as it appears in published clinical or preclinical research and official regulatory documents. It is provided as published-literature reference material. It is not dosing guidance, not medical advice, and not a recommendation to use or self-administer this compound.
Raloxifene is an FDA-approved prescription medicine, sold as Evista. According to the FDA-approved labeling, the dose for both the prevention and the treatment of postmenopausal osteoporosis is 60 mg once daily, taken at any time of day with or without food, alongside adequate calcium and vitamin D intake. The 60 mg dose was the dose evaluated in the pivotal MORE osteoporosis trial. These figures are drawn from FDA-approved prescribing information.
Important
Raloxifene carries an FDA Boxed Warning for an increased risk of venous thromboembolism and of death from stroke in certain populations. The labeled dose applies to the approved prescription product used under medical supervision; it is not a recommendation and does not apply to material sold for research use.
Safety and Side Effects
Raloxifene is an FDA-approved drug, and it carries an FDA boxed warning, the agency’s most serious warning category. The boxed warning addresses two serious risks: an increased risk of venous thromboembolism, meaning deep vein thrombosis and pulmonary embolism, and an increased risk of death due to stroke in women with documented coronary heart disease or at increased risk for major coronary events. For this reason raloxifene is contraindicated in women with a history of venous thromboembolic events. The most common adverse effects are hot flashes and leg cramps. Because of the thrombosis risk, the drug is generally stopped before and during prolonged immobilization, such as around surgery.
Current Research Status
Raloxifene is an FDA-approved prescription medication, marketed as Evista, approved for the prevention and treatment of osteoporosis in postmenopausal women and for reducing the risk of invasive breast cancer in certain postmenopausal women. As a prescription drug with a boxed warning, it should be used only under medical supervision and after individual assessment of cardiovascular and thrombosis risk.
Further reading: For a related SERM studied in the context of testosterone support, see Enclomiphene: The SERM Studied for Testosterone.
Frequently Asked Questions
What is raloxifene?
Raloxifene, brand name Evista, is a second-generation selective estrogen receptor modulator (SERM). It is an FDA-approved prescription medicine, approved in 1997, used to prevent and treat postmenopausal osteoporosis and to reduce breast cancer risk in certain women.
How does raloxifene work?
Raloxifene binds estrogen receptors but induces a receptor conformation different from estrogen’s. This makes it selective: it acts like estrogen in bone, helping preserve bone density, while blocking estrogen’s effect in breast tissue.
Is raloxifene FDA-approved?
Yes. Raloxifene is FDA-approved for the prevention and treatment of osteoporosis in postmenopausal women and for reducing the risk of invasive breast cancer in certain postmenopausal women.
What does the research say about raloxifene?
The pivotal MORE trial (1999), a randomized, placebo-controlled study in 7,705 postmenopausal women with osteoporosis, found that raloxifene 60 mg daily reduced the risk of vertebral fractures over three years. It has long-term clinical data.
What are the safety concerns with raloxifene?
Raloxifene carries an FDA boxed warning addressing two serious risks: an increased risk of venous thromboembolism (deep vein thrombosis and pulmonary embolism) and an increased risk of death due to stroke in women with certain cardiovascular risk factors.
Research Handling & Storage
Storage
- Unopened: Store at controlled room temperature, 20–25°C (68–77°F), away from direct sunlight, heat, and moisture.
- Opened: Keep container tightly closed. Use within the timeframe indicated on the label, typically 30–90 days after opening.
- Do not freeze liquid solutions unless specifically indicated.
Handling Precautions
- Handle with appropriate personal protective equipment (PPE) including nitrile gloves, lab coat, and eye protection.
- Use aseptic/sterile technique when reconstituting and transferring solutions to prevent contamination.
- Avoid repeated freeze-thaw cycles which may denature the compound and reduce potency.
- Keep detailed laboratory records including reconstitution dates, lot numbers, concentrations, and storage conditions.
- Dispose of unused material and sharps in accordance with local regulations and institutional biosafety guidelines.
Stability & Shelf Life
Liquid formulations typically remain stable for 1–2 years when stored at the recommended temperature in the original sealed container. Once opened, potency may gradually decrease. Monitor for any changes in color, clarity, or odor, which may indicate degradation.
Purity & Quality Considerations
Research-grade compounds should be accompanied by a Certificate of Analysis (COA) confirming purity, typically verified by High-Performance Liquid Chromatography (HPLC) and Mass Spectrometry (MS). Look for purity levels of ≥98% for research applications. Third-party testing adds an additional layer of quality assurance. Always verify the source and documentation before using any research compound.
Research Supplies & Resources
Essential supplies and educational resources for peptide research. Links go to Amazon.com.
Lab Supplies
Recommended Reading
Lab Equipment
As an Amazon Associate, peptides.fyi earns from qualifying purchases. Learn more.