Synopsis
Compound overview
- Research only
- In clinical trials
- Approved outside US
- FDA-approved
What it is
Pramipexole is a dopamine agonist. It is an FDA-approved prescription medicine, used to treat Parkinson's disease and restless legs syndrome.
What it does
Documented uses include:
- Treats Parkinson's disease symptoms
- Treats restless legs syndrome
- Studied for mood-related effects
- Has long-standing clinical data
How it works
Pramipexole activates dopamine receptors in the brain, partly making up for the loss of dopamine signalling that drives Parkinson's symptoms.
Safety notes
Pramipexole is prescription-only. It is known for unusual but serious side effects, including sudden sleep attacks and impulse-control problems such as compulsive gambling or shopping. It should only be used under medical supervision; research-vendor material is not pharmacy-grade.
Where to buy Pramipexole
Standard lyophilized vial — reconstitute and measure doses yourself. The conventional research format.
Affiliate links — we may earn a commission at no extra cost to you.
Molecular Structure
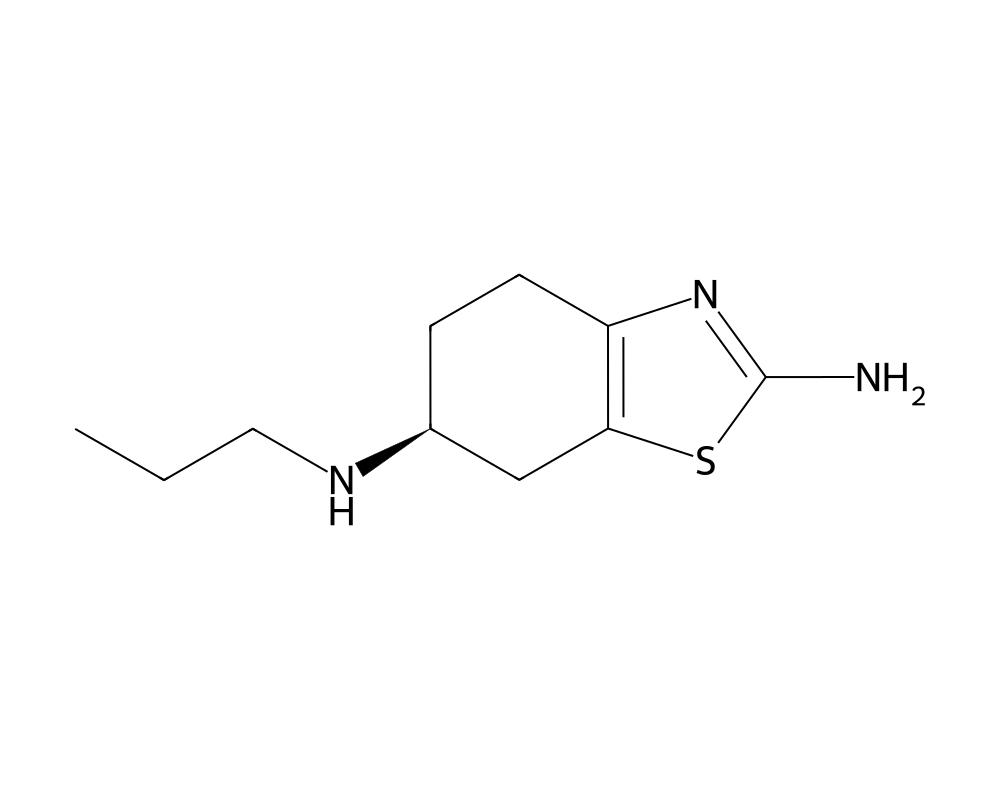
Overview
Pramipexole is a non-ergot dopamine receptor agonist belonging to the aminobenzothiazole class of compounds. Developed by Boehringer Ingelheim and marketed under the brand name Mirapex, it was approved by the FDA in 1997 for the treatment of idiopathic Parkinson’s disease and subsequently in 2006 for moderate to severe restless legs syndrome (RLS). Pramipexole is available in both immediate-release and extended-release (Mirapex ER) formulations.
Contents
- Overview
- Mechanism of Action
- Motor Symptom Control in Parkinson's Disease
- D3 Receptor Preferential Activity
- Potential Neuroprotective Properties
- Research Summary
- Shannon et al. (1997) – Parkinson's Disease
- Hubble et al. (1995) – Early Clinical Development
- Restless Legs Syndrome
- Dosing in Published Research
- Safety and Side Effects
- Current Research Status
- Frequently Asked Questions
Pramipexole is distinguished from other dopamine agonists by its high selectivity for the D3 subfamily of dopamine D2-like receptors. The D3 receptor is preferentially expressed in limbic brain regions, including the nucleus accumbens, ventral tegmental area, and islands of Calleja, as well as in the substantia nigra. This receptor distribution pattern is significant because D3 receptors are believed to play important roles in mood regulation, motivation, reward processing, and neuroprotection, in addition to motor function.
As a non-ergot dopamine agonist, pramipexole does not carry the risk of fibrotic complications (retroperitoneal, pulmonary, and cardiac valve fibrosis) associated with ergot-derived dopamine agonists such as bromocriptine, cabergoline, and pergolide. This improved safety profile, combined with its efficacy and once-daily extended-release formulation, has made pramipexole one of the most widely prescribed dopamine agonists worldwide.
Mechanism of Action
Pramipexole acts as a full agonist at dopamine D2-family receptors (D2, D3, and D4), with preferential binding affinity for the D3 receptor subtype. Its intrinsic activity at these receptors mimics the actions of endogenous dopamine, providing symptomatic relief in conditions characterized by dopaminergic deficiency.
Motor Symptom Control in Parkinson’s Disease
In Parkinson’s disease, the progressive degeneration of dopaminergic neurons in the substantia nigra pars compacta leads to dopamine depletion in the dorsal striatum (caudate nucleus and putamen). Pramipexole directly stimulates postsynaptic D2 and D3 receptors in the striatum, bypassing the need for presynaptic dopamine synthesis, storage, and release. This direct receptor activation restores inhibitory signaling in the indirect pathway of the basal ganglia circuitry, reducing the excessive inhibitory output from the globus pallidus internus/substantia nigra pars reticulata to the thalamus that underlies parkinsonian bradykinesia and rigidity.
D3 Receptor Preferential Activity
Pramipexole binds to the D3 receptor with approximately 7-fold greater affinity than to the D2 receptor (Ki of 0.5 nM vs. 3.9 nM, respectively). The D3 receptor’s predominant expression in mesolimbic and mesocortical circuits suggests that D3-mediated effects contribute to pramipexole’s reported benefits on depression, anhedonia, and apathy in Parkinson’s disease patients, as well as its efficacy in restless legs syndrome. However, the D3 receptor’s role in reward circuitry also underlies the concerning association between pramipexole use and impulse control disorders, including pathological gambling, compulsive shopping, and hypersexuality.
Potential Neuroprotective Properties
Preclinical studies have suggested that pramipexole may possess neuroprotective properties independent of its dopamine receptor agonism. In vitro studies have demonstrated that pramipexole can scavenge reactive oxygen species, reduce oxidative stress, and inhibit the opening of the mitochondrial permeability transition pore, a critical event in apoptotic cell death. Additionally, pramipexole has been shown to upregulate expression of brain-derived neurotrophic factor (BDNF) in animal models. However, these neuroprotective effects have not been conclusively demonstrated in clinical trials.
Research Summary
Shannon et al. (1997) – Parkinson’s Disease
Shannon et al. (1997) published results from a pivotal double-blind, placebo-controlled trial evaluating pramipexole in early Parkinson’s disease. The study demonstrated significant improvements in the Unified Parkinson’s Disease Rating Scale (UPDRS) motor score with pramipexole compared to placebo. Patients receiving pramipexole showed dose-dependent improvements of 20-31% in motor function scores at doses of 1.5-6.0 mg/day. The study established the efficacy of pramipexole as monotherapy in early Parkinson’s disease and defined the effective dose range.
Hubble et al. (1995) – Early Clinical Development
Hubble et al. (1995) reported early clinical data on pramipexole’s pharmacological profile and initial efficacy observations in Parkinson’s disease patients. This foundational work characterized the dose-response relationship, pharmacokinetic parameters, and preliminary safety profile of the compound. The study demonstrated that pramipexole was well absorbed orally with a bioavailability greater than 90%, was minimally metabolized (excreted largely unchanged by the kidneys), and had a terminal elimination half-life of approximately 8-12 hours, supporting three-times-daily dosing with the immediate-release formulation.
Restless Legs Syndrome
Multiple randomized controlled trials have established pramipexole’s efficacy in moderate to severe restless legs syndrome. Studies demonstrated significant improvements in the International Restless Legs Syndrome Study Group (IRLS) rating scale, with optimal efficacy at doses of 0.25-0.50 mg taken 2-3 hours before bedtime. However, long-term treatment with dopamine agonists for RLS has been associated with augmentation, a paradoxical worsening of symptoms with chronic therapy, leading to evolving clinical guidelines regarding duration of treatment.
Dosing in Published Research
About this section
The information below reports dosing only as it appears in published clinical or preclinical research and official regulatory documents. It is provided as published-literature reference material. It is not dosing guidance, not medical advice, and not a recommendation to use or self-administer this compound.
Pramipexole is an FDA-approved prescription medicine, sold as Mirapex. Its labeled dosing differs by indication:
- Parkinson disease: the FDA-approved labeling describes gradual titration from a starting dose of 0.375 mg per day up to a maximum of 4.5 mg per day.
- Restless legs syndrome: a single dose between 0.125 mg and 0.5 mg taken 2 to 3 hours before bedtime.
These figures are drawn from FDA-approved prescribing information.
Important
Pramipexole has been associated with sudden onset of sleep and with impulse-control disorders such as compulsive gambling. The doses above apply to the approved prescription product used under medical supervision; they are not a recommendation and do not apply to material sold for research use.
Safety and Side Effects
The most clinically significant risk associated with pramipexole, and with dopamine agonists as a class, is the development of impulse-control disorders. Pathological gambling, compulsive shopping, hypersexuality, and binge eating have been documented in patients taking pramipexole, sometimes emerging without warning and without the patient recognizing the behavior as drug-related. These behaviors can have severe financial, legal, and personal consequences, and they have been the subject of extensive litigation. The risk is dose-related but can occur at therapeutic doses, and behaviors typically resolve when the drug is reduced or stopped. A related phenomenon, dopamine dysregulation syndrome, involves compulsive overuse of dopaminergic medication.
Pramipexole can cause sudden-onset sleep, including episodes of falling asleep during activities of daily living such as driving, sometimes without any preceding sense of drowsiness. Patients are advised not to drive or operate machinery until they know how the drug affects them. Orthostatic hypotension, with lightheadedness or fainting on standing, is common, particularly during dose initiation and titration. Hallucinations and other psychotic symptoms can occur, more often in older patients and those with Parkinson’s disease. Other reported effects include nausea, constipation, peripheral edema, dizziness, and dyskinesia. Abrupt discontinuation can provoke a withdrawal syndrome (dopamine agonist withdrawal syndrome) with anxiety, depression, pain, and autonomic symptoms, so the drug should be tapered under medical supervision.
Current Research Status
Pramipexole is an FDA-approved prescription medication, indicated for Parkinson’s disease and for moderate to severe primary restless legs syndrome. It is a well-studied drug with decades of clinical use and a clearly characterized adverse-effect profile. It is not approved for any performance, cognitive, or mood-enhancement use; investigation of pramipexole in depression has occurred but it carries no such approved indication. As a prescription drug with significant behavioral and cardiovascular risks, pramipexole should be used only under medical supervision. Pramipexole appears in the Performance category on this site for grouping convenience only; this is not a recommendation of any performance use.
Frequently Asked Questions
What is pramipexole?
Pramipexole is a non-ergot dopamine receptor agonist. It is an FDA-approved prescription medicine, approved in 1997, used to treat Parkinson’s disease and, later, moderate to severe restless legs syndrome.
How does pramipexole work?
Pramipexole activates dopamine D2-family receptors, with a preference for the D3 subtype, mimicking the action of natural dopamine. This partly compensates for the loss of dopamine signalling that drives Parkinson’s symptoms.
Is pramipexole FDA-approved?
Yes. Pramipexole is an FDA-approved prescription medication indicated for Parkinson’s disease and for moderate to severe primary restless legs syndrome, with decades of clinical use. It is not approved for performance or cognitive enhancement.
What does the research say about pramipexole?
A pivotal double-blind, placebo-controlled trial by Shannon and colleagues (1997) showed significant improvement in motor symptoms in early Parkinson’s disease. It has long-standing clinical data across its approved indications and has also been studied for mood-related effects.
What are the safety concerns with pramipexole?
The most clinically significant risk, shared across dopamine agonists, is impulse-control disorders such as pathological gambling, compulsive shopping, hypersexuality and binge eating. It is a prescription medicine that should be used only under medical supervision.
Research Handling & Storage
Storage
- Unopened: Store at controlled room temperature, 20–25°C (68–77°F), away from direct sunlight, heat, and moisture.
- Opened: Keep container tightly closed. Use within the timeframe indicated on the label, typically 30–90 days after opening.
- Do not freeze liquid solutions unless specifically indicated.
Handling Precautions
- Handle with appropriate personal protective equipment (PPE) including nitrile gloves, lab coat, and eye protection.
- Use aseptic/sterile technique when reconstituting and transferring solutions to prevent contamination.
- Avoid repeated freeze-thaw cycles which may denature the compound and reduce potency.
- Keep detailed laboratory records including reconstitution dates, lot numbers, concentrations, and storage conditions.
- Dispose of unused material and sharps in accordance with local regulations and institutional biosafety guidelines.
Stability & Shelf Life
Liquid formulations typically remain stable for 1–2 years when stored at the recommended temperature in the original sealed container. Once opened, potency may gradually decrease. Monitor for any changes in color, clarity, or odor, which may indicate degradation.
Purity & Quality Considerations
Research-grade compounds should be accompanied by a Certificate of Analysis (COA) confirming purity, typically verified by High-Performance Liquid Chromatography (HPLC) and Mass Spectrometry (MS). Look for purity levels of ≥98% for research applications. Third-party testing adds an additional layer of quality assurance. Always verify the source and documentation before using any research compound.
Research Supplies & Resources
Essential supplies and educational resources for peptide research. Links go to Amazon.com.
Lab Supplies
Recommended Reading
Lab Equipment
As an Amazon Associate, peptides.fyi earns from qualifying purchases. Learn more.