Synopsis
Compound overview
- Research only
- In clinical trials
- Approved outside US
- FDA-approved
What it is
L-carnitine is a compound the body makes from amino acids and also gets from food, mainly meat. It is sold widely as a supplement, and a prescription form (levocarnitine) is FDA-approved to treat genuine carnitine deficiency.
What it does
Recognised and studied roles include:
- Helps the body turn fat into usable energy
- Prescription form treats carnitine deficiency
- Studied for exercise and recovery
- Researched for heart and metabolic health
How it works
L-carnitine carries fatty acids into the mitochondria — the part of the cell where fat is burned for energy — so it plays a direct role in how the body uses fat as fuel.
Safety notes
L-carnitine is generally well tolerated; high doses can cause nausea, stomach upset and a fishy body odour. Some research has linked a carnitine breakdown product (TMAO) to cardiovascular risk, so the picture for heart health is not settled. The prescription form should be used under medical care.
Where to buy L-Carnitine
Standard lyophilized vial — reconstitute and measure doses yourself. The conventional research format.
Affiliate links — we may earn a commission at no extra cost to you.
Molecular Structure
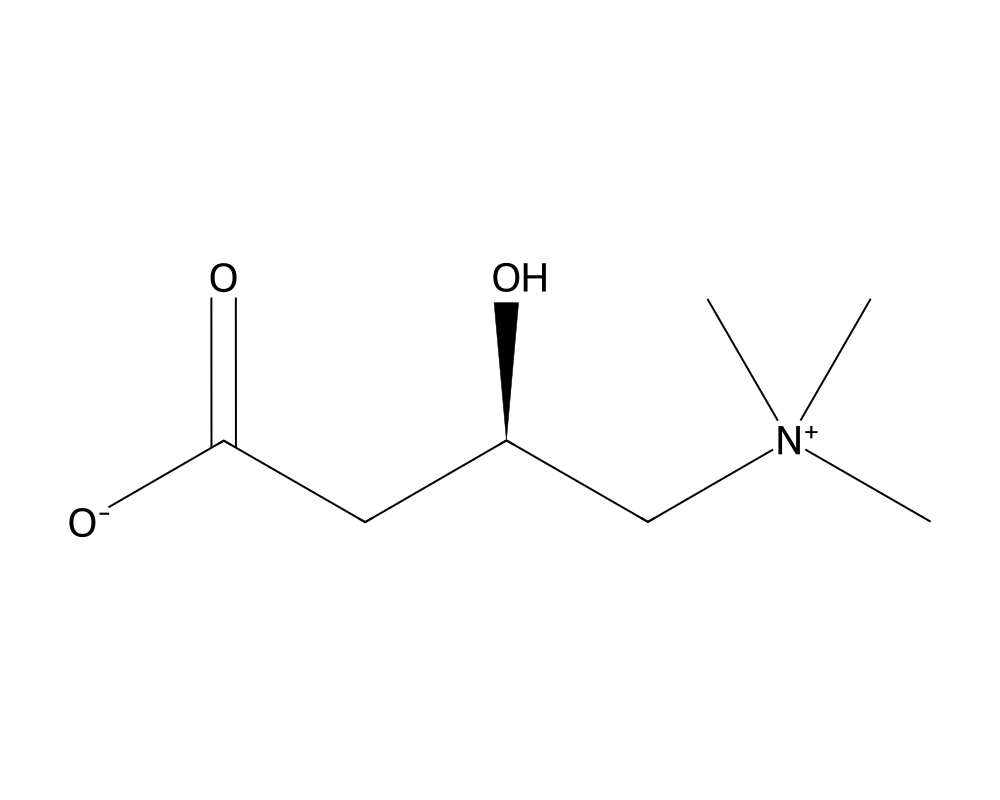
Overview
L-Carnitine is a naturally occurring quaternary ammonium compound biosynthesized from the essential amino acids lysine and methionine. It plays an indispensable role in cellular energy metabolism by facilitating the transport of long-chain fatty acids across the inner mitochondrial membrane for beta-oxidation. First isolated from meat extract in 1905 by Gulewitsch and Krimberg, L-carnitine was identified as an essential cofactor for fatty acid oxidation by Fritz in 1963.
Contents
- Overview
- Mechanism of Action
- The Carnitine Shuttle
- Regulation of the Acyl-CoA/CoA Ratio
- Acetyl-L-Carnitine and Neuroprotection
- Research Summary
- Pekala et al. (2011) – Comprehensive Review
- Malaguarnera et al. (2010) – Hepatic Steatosis
- Exercise Performance and Recovery
- Dosing in Published Research
- Safety and Side Effects
- Current Research Status
- Frequently Asked Questions
In humans, approximately 75% of carnitine is obtained from dietary sources (primarily red meat, dairy, and fish), with the remainder synthesized endogenously in the liver, kidneys, and brain from lysine and methionine in a reaction requiring vitamin C, vitamin B6, niacin, and iron. The total body pool of carnitine in adults is approximately 20 grams, with more than 95% concentrated in skeletal and cardiac muscle. Plasma carnitine levels are tightly regulated by renal reabsorption, with the kidneys reclaiming approximately 95% of filtered carnitine under normal conditions.
L-Carnitine is available both as a dietary supplement in several forms (L-carnitine tartrate, acetyl-L-carnitine, propionyl-L-carnitine) and as a prescription medication (Carnitor/levocarnitine) for the treatment of primary and secondary carnitine deficiency. The various supplemental forms have different pharmacokinetic properties and tissue distribution patterns, which has led to their use in different clinical and research contexts.
Mechanism of Action
L-Carnitine’s primary biochemical function is the facilitation of long-chain fatty acid transport into the mitochondrial matrix, where beta-oxidation occurs. This transport process, known as the carnitine shuttle, is essential because the inner mitochondrial membrane is impermeable to long-chain fatty acyl-CoA esters.
The Carnitine Shuttle
The carnitine shuttle operates through three enzymatic steps. First, carnitine palmitoyltransferase I (CPT-I), located on the outer mitochondrial membrane, catalyzes the transfer of the acyl group from coenzyme A to carnitine, forming acylcarnitine. Second, carnitine-acylcarnitine translocase (CACT), an integral inner membrane protein, exchanges acylcarnitine for free carnitine across the inner mitochondrial membrane. Third, carnitine palmitoyltransferase II (CPT-II), located on the matrix side of the inner membrane, regenerates acyl-CoA from acylcarnitine, releasing free carnitine to recycle back through the translocase. The acyl-CoA then enters the beta-oxidation spiral, generating acetyl-CoA for the citric acid cycle and reducing equivalents (FADH2, NADH) for oxidative phosphorylation.
Regulation of the Acyl-CoA/CoA Ratio
Beyond its shuttle function, L-carnitine serves as a buffer for the intracellular acyl-CoA/free CoA ratio. By accepting acyl groups from acyl-CoA, carnitine frees coenzyme A for participation in other metabolic reactions, including the pyruvate dehydrogenase complex (linking glycolysis to the citric acid cycle). This buffering function is particularly important during high metabolic demand or in pathological states where acyl-CoA accumulation could impair multiple metabolic pathways.
Acetyl-L-Carnitine and Neuroprotection
Acetyl-L-carnitine (ALCAR), the acetylated form, crosses the blood-brain barrier more efficiently than unesterified L-carnitine and serves as a donor of acetyl groups for acetylcholine synthesis. ALCAR has been investigated for neuroprotective and neurotrophic properties, including upregulation of nerve growth factor (NGF) receptors, stabilization of mitochondrial membrane potential, and reduction of oxidative stress markers in neural tissue. These properties have led to clinical investigations in age-related cognitive decline, peripheral neuropathy, and neurodegenerative diseases.
Research Summary
Pekala et al. (2011) – Comprehensive Review
Pekala et al. (2011) published a comprehensive review of L-carnitine’s biochemistry, pharmacokinetics, and clinical applications in Current Drug Metabolism. The review synthesized evidence from hundreds of studies documenting L-carnitine’s role in fatty acid oxidation, its pharmacokinetic profile (oral bioavailability of 5-18% for L-carnitine supplements, higher for acetyl-L-carnitine), and its clinical applications spanning primary carnitine deficiency, secondary deficiency states (hemodialysis, valproic acid therapy), cardiovascular disease, diabetes, and neurological conditions. The review highlighted that while L-carnitine deficiency clearly causes metabolic dysfunction, the evidence for supplementation benefit in carnitine-replete individuals remained mixed.
Malaguarnera et al. (2010) – Hepatic Steatosis
Malaguarnera et al. (2010) conducted a randomized, double-blind, placebo-controlled trial evaluating L-carnitine supplementation in patients with non-alcoholic steatohepatitis (NASH), published in the American Journal of Gastroenterology. The study enrolled 74 patients randomized to L-carnitine 2 g/day or placebo for 24 weeks. L-carnitine supplementation produced significant improvements in liver enzymes (AST, ALT, GGT), inflammatory markers (TNF-alpha, CRP), insulin resistance (HOMA-IR), and histological measures of steatosis, necroinflammation, and fibrosis compared to placebo. These findings supported the hypothesis that enhancing fatty acid oxidation through carnitine supplementation could ameliorate hepatic lipid accumulation.
Exercise Performance and Recovery
The effect of L-carnitine on exercise performance has been extensively studied with mixed results. While carnitine supplementation does not appear to enhance fat oxidation or exercise performance in well-nourished athletes under most conditions, Wall et al. (2011) demonstrated that chronic L-carnitine supplementation combined with carbohydrate loading could increase muscle carnitine content by 21% and improve exercise efficiency. L-carnitine L-tartrate has also shown promise in reducing markers of exercise-induced muscle damage and improving recovery between training sessions.
Dosing in Published Research
About this section
The information below reports dosing only as it appears in published clinical or preclinical research and official regulatory documents. It is provided as published-literature reference material. It is not dosing guidance, not medical advice, and not a recommendation to use or self-administer this compound.
L-carnitine, as levocarnitine, is an FDA-approved prescription medicine, sold as Carnitor, for primary carnitine deficiency and for certain secondary deficiencies. According to the FDA-approved labeling, dosing depends on the formulation:
- Oral tablets: 990 mg taken two or three times daily.
- Oral solution: 1 to 3 g per day for a 50 kg patient, adjusted to the individual.
- Intravenous injection: 50 mg per kg, with dosing individualized in metabolic crisis.
These figures are drawn from FDA-approved prescribing information. L-carnitine is also widely sold as a dietary supplement, a use that is not covered by this drug labeling.
Important
The figures above describe the approved prescription product used to treat diagnosed carnitine deficiency under medical supervision. They are not a recommendation, and they do not establish a dose for performance, weight-loss, or general supplemental use.
Safety and Side Effects
L-carnitine is a naturally occurring amino acid derivative available as a dietary supplement, and at typical supplement doses it is generally well tolerated. Higher doses can cause gastrointestinal effects such as nausea, cramping, and diarrhea, and a characteristic fishy body odor. A more substantive concern emerging from research is metabolic: gut bacteria convert L-carnitine to trimethylamine, which the liver oxidizes to trimethylamine-N-oxide (TMAO), a metabolite that observational and mechanistic studies have associated with atherosclerosis and cardiovascular risk. The clinical significance of supplemental L-carnitine and TMAO for cardiovascular outcomes is still debated and not settled. Injectable L-carnitine and the prescription form used for diagnosed carnitine deficiency are separate from over-the-counter supplements and should be used under medical guidance.
Current Research Status
L-carnitine in its common over-the-counter form is regulated as a dietary supplement; a prescription form, levocarnitine, is FDA-approved for primary and certain secondary carnitine-deficiency states. It is not an approved drug for weight loss, athletic performance, or general enhancement, and the evidence for those uses is mixed. L-carnitine appears in the Performance category on this site for grouping convenience only; this is not a recommendation of any performance use.
Frequently Asked Questions
What is L-carnitine?
L-carnitine is a compound the body makes from the amino acids lysine and methionine and also obtains from food, mainly meat. It is sold widely as a dietary supplement, and a prescription form, levocarnitine, is FDA-approved to treat genuine carnitine deficiency.
How does L-carnitine work?
L-carnitine carries long-chain fatty acids across the inner mitochondrial membrane so they can be burned for energy, a process known as the carnitine shuttle. This role is essential for the cell’s use of fat as fuel.
Is L-carnitine FDA-approved?
The common over-the-counter form is regulated as a dietary supplement, not an approved drug. A prescription form, levocarnitine, is FDA-approved specifically for primary and certain secondary carnitine-deficiency states.
What does the research say about L-carnitine?
Its role in fatty-acid metabolism and deficiency treatment is well documented. Research has also examined L-carnitine for exercise, recovery and heart and metabolic health, but evidence for benefit in people without a deficiency is mixed.
What are the safety concerns with L-carnitine?
At typical supplement doses L-carnitine is generally well tolerated. Higher doses can cause gastrointestinal effects such as nausea, cramping and diarrhea, and a characteristic fishy body odor. It is not an approved treatment for weight loss or athletic performance.
Research Handling & Storage
Storage
- Unopened: Store at controlled room temperature, 20–25°C (68–77°F), away from direct sunlight, heat, and moisture.
- Opened: Keep container tightly closed. Use within the timeframe indicated on the label, typically 30–90 days after opening.
- Do not freeze liquid solutions unless specifically indicated.
Handling Precautions
- Handle with appropriate personal protective equipment (PPE) including nitrile gloves, lab coat, and eye protection.
- Use aseptic/sterile technique when reconstituting and transferring solutions to prevent contamination.
- Avoid repeated freeze-thaw cycles which may denature the compound and reduce potency.
- Keep detailed laboratory records including reconstitution dates, lot numbers, concentrations, and storage conditions.
- Dispose of unused material and sharps in accordance with local regulations and institutional biosafety guidelines.
Stability & Shelf Life
Liquid formulations typically remain stable for 1–2 years when stored at the recommended temperature in the original sealed container. Once opened, potency may gradually decrease. Monitor for any changes in color, clarity, or odor, which may indicate degradation.
Purity & Quality Considerations
Research-grade compounds should be accompanied by a Certificate of Analysis (COA) confirming purity, typically verified by High-Performance Liquid Chromatography (HPLC) and Mass Spectrometry (MS). Look for purity levels of ≥98% for research applications. Third-party testing adds an additional layer of quality assurance. Always verify the source and documentation before using any research compound.
Research Supplies & Resources
Essential supplies and educational resources for peptide research. Links go to Amazon.com.
Lab Supplies
Recommended Reading
Lab Equipment
As an Amazon Associate, peptides.fyi earns from qualifying purchases. Learn more.