Synopsis
Compound overview
- Research only
- In clinical trials
- Approved outside US
- FDA-approved
What it is
Liothyronine is a synthetic form of T3, the more active thyroid hormone. It is an FDA-approved prescription medicine, sold as Cytomel to treat an underactive thyroid and other thyroid conditions.
What it does
Documented and misused applications include:
- Treats hypothyroidism (underactive thyroid)
- Used in some thyroid diagnostic tests
- Sometimes misused for weight loss
- Acts faster than the standard thyroid drug levothyroxine
How it works
Liothyronine directly supplies T3, the thyroid hormone that sets the body's metabolic rate, bypassing the body's normal conversion of T4 into T3.
Safety notes
Liothyronine is prescription-only and dosing must be precise. Too much causes a racing heart, anxiety, bone loss and heart-rhythm problems, which is why using it for weight loss is dangerous. It should only be used under medical supervision; research-vendor material is not pharmacy-grade.
Where to buy Liothyronine (T3)
Standard lyophilized vial — reconstitute and measure doses yourself. The conventional research format.
Affiliate links — we may earn a commission at no extra cost to you.
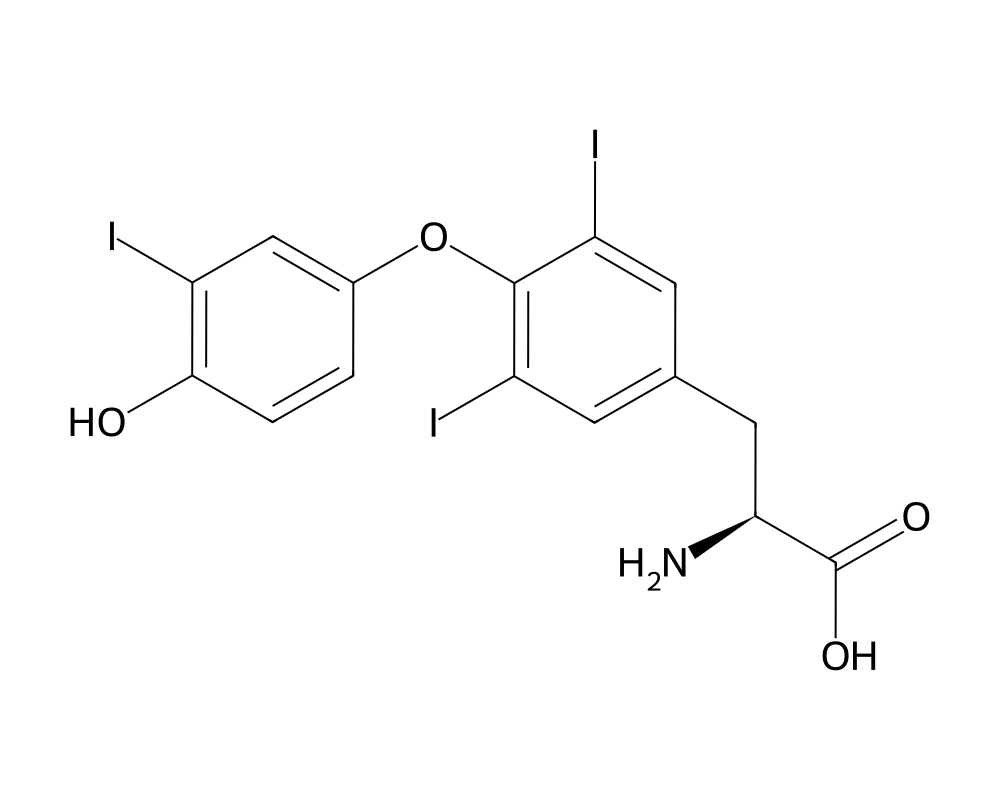
Molecular Structure
Research tool
Reconstitution calculator
Concentration
2.50mg/mL
Draw volume
0.10mL
Insulin units
10IU
Doses/vial
20
Overview
Liothyronine is the synthetic form of triiodothyronine (T3), the most biologically active thyroid hormone produced by the human body. Marketed under brand names including Cytomel and Triostat, liothyronine has been used clinically since the 1950s for the treatment of hypothyroidism, myxedema coma, and as a diagnostic agent in thyroid suppression tests. While levothyroxine (synthetic T4) has become the standard of care for hypothyroidism due to its longer half-life and more stable pharmacokinetics, liothyronine retains an important role in clinical practice and continues to generate significant research interest.
Contents
The distinction between T3 and T4 is fundamental to thyroid physiology. The thyroid gland produces predominantly T4, which functions as a prohormone. Peripheral tissues convert T4 to T3 through the action of deiodinase enzymes. T3 binds to nuclear thyroid hormone receptors with approximately 10 times greater affinity than T4, making it the primary mediator of thyroid hormone action at the cellular level. Liothyronine delivers this active hormone directly, bypassing the conversion step entirely.
Mechanism of Action
Liothyronine enters target cells through specific membrane transporters, including monocarboxylate transporter 8 (MCT8) and organic anion transporting polypeptide 1C1 (OATP1C1). Once inside the cell, it binds to thyroid hormone receptors (TR-alpha and TR-beta) in the nucleus. These receptors function as ligand-activated transcription factors, binding to thyroid hormone response elements (TREs) in the promoter regions of target genes.
The genomic effects of T3 are remarkably broad. Thyroid hormone receptor activation influences the transcription of genes involved in basal metabolic rate, thermogenesis, protein synthesis, lipid metabolism, carbohydrate metabolism, and cardiac function. In mitochondria, T3 stimulates oxidative phosphorylation and increases oxygen consumption. The net physiological effect is an increase in metabolic rate across virtually every tissue in the body.
T3 also exerts rapid, non-genomic effects through interactions with membrane-associated receptors and cytoplasmic signaling pathways. These include acute effects on cardiac contractility, vascular tone, and ion channel function that occur too quickly to be explained by changes in gene transcription. The interplay between genomic and non-genomic actions contributes to the complex pharmacodynamic profile of exogenous liothyronine.
Critically, exogenous T3 administration suppresses the HPT (hypothalamic-pituitary-thyroid) axis. Elevated T3 levels inhibit hypothalamic TRH and pituitary TSH secretion, reducing endogenous thyroid hormone production. This negative feedback loop means that supraphysiological T3 dosing will progressively suppress native thyroid function, a consideration of paramount importance in research contexts.
Research Summary
Clinical research on liothyronine spans multiple domains. In the treatment of hypothyroidism, the most active area of investigation concerns combination T4/T3 therapy versus T4 monotherapy. Despite normal TSH levels on levothyroxine alone, a subset of hypothyroid patients report persistent symptoms including fatigue, cognitive difficulties, and mood disturbances. Multiple randomized controlled trials have examined whether adding liothyronine to levothyroxine improves these symptoms, with mixed but increasingly nuanced results.
A 2018 meta-analysis published in the Journal of Clinical Endocrinology and Metabolism found that combination therapy was associated with modest improvements in patient preference and certain quality-of-life measures, though objective neurocognitive outcomes were not consistently improved. Genetic studies have identified that polymorphisms in the DIO2 gene, which encodes the type 2 deiodinase enzyme responsible for T4-to-T3 conversion, may predict which patients benefit from combination therapy. This pharmacogenomic approach represents a frontier in personalized thyroid treatment.
In the context of metabolic research, liothyronine has been studied for its effects on body composition and energy expenditure. Short-term studies demonstrate reliable increases in resting metabolic rate, with doses as low as 25 mcg daily producing measurable thermogenic effects. However, the catabolic nature of T3 at supraphysiological levels means that weight loss is not limited to fat mass; muscle protein catabolism increases as well. Research on thyroid hormone analogs with tissue-selective activity aims to capture the metabolic benefits while minimizing muscle wasting and cardiac effects.
Liothyronine’s role in the management of treatment-resistant depression has been studied for decades. Augmentation of antidepressant therapy with low-dose T3 (25 to 50 mcg daily) has shown efficacy in several trials, most notably in the STAR*D study, where it performed comparably to lithium augmentation. The mechanism underlying this psychiatric effect remains incompletely understood but may involve T3’s influence on serotonergic and noradrenergic neurotransmission.
Dosing in Published Research
About this section
The information below reports dosing only as it appears in published clinical or preclinical research and official regulatory documents. It is provided as published-literature reference material. It is not dosing guidance, not medical advice, and not a recommendation to use or self-administer this compound.
Liothyronine is the synthetic form of the thyroid hormone T3 and is an FDA-approved prescription medicine, sold as Cytomel. According to the FDA-approved labeling for hypothyroidism, the usual starting dose is 25 mcg daily, which may be increased by up to 25 mcg every 1 to 2 weeks; the usual maintenance dose is 25 to 75 mcg daily. For elderly patients or those with cardiac disease, labeling advises starting at 5 mcg daily. These figures are drawn from FDA-approved prescribing information.
Important
Thyroid hormone preparations, including liothyronine, carry an FDA Boxed Warning against use for the treatment of obesity or for weight loss; in euthyroid people, doses within or above the normal range can cause serious and even life-threatening toxicity. The doses above apply to the approved prescription product used to treat diagnosed hypothyroidism under medical supervision; they are not a recommendation and do not apply to material sold for research use.
Safety and Side Effects
The side effects of liothyronine are largely predictable extensions of its pharmacological action. At excessive doses, symptoms of thyrotoxicosis emerge: tachycardia, palpitations, tremor, anxiety, insomnia, heat intolerance, diarrhea, and unintentional weight loss. Cardiac effects are the most clinically significant concern, as T3 directly increases heart rate, cardiac output, and myocardial oxygen demand. Atrial fibrillation is a recognized risk with sustained supraphysiological T3 levels, particularly in older individuals and those with preexisting cardiac disease.
Bone mineral density loss is another well-documented consequence of excess thyroid hormone exposure. T3 stimulates osteoclast activity and increases bone remodeling, and sustained overreplacement is associated with decreased bone density, particularly at cortical sites. This risk is most pronounced in postmenopausal women.
The short half-life of liothyronine (approximately 24 hours) produces wider fluctuations in serum T3 levels compared to the stable levels achieved with levothyroxine. Peak T3 concentrations occur two to four hours after oral dosing and may transiently exceed the normal range even at replacement doses, potentially producing symptomatic hyperthyroid episodes. This pharmacokinetic characteristic is both a limitation for chronic therapy and a reason for ongoing interest in sustained-release T3 formulations.
HPT axis suppression following prolonged use at supraphysiological doses is a significant concern in research settings. Recovery of normal thyroid function after exogenous T3 withdrawal can take weeks to months, and some investigators have questioned whether prolonged suppression may cause lasting changes in thyroid gland function.
Current Research Status
Liothyronine is an FDA-approved medication with decades of clinical experience. Active areas of research include the development of sustained-release T3 formulations, pharmacogenomic approaches to identifying patients who benefit from combination T4/T3 therapy, and thyroid hormone analogs with improved tissue selectivity. Research into T3 augmentation for psychiatric conditions and its role in critical care settings (such as euthyroid sick syndrome) continues to generate new data. The compound remains indispensable as both a clinical therapeutic and a research tool for studying thyroid hormone biology.
Frequently Asked Questions
What is liothyronine (T3)?
Liothyronine is a synthetic form of triiodothyronine (T3), the most biologically active thyroid hormone. Sold under brand names such as Cytomel, it is an FDA-approved prescription medicine used since the 1950s to treat hypothyroidism and related conditions.
How does liothyronine work?
Liothyronine directly supplies T3, which enters cells through specific transporters and binds thyroid hormone receptors in the cell nucleus. These receptors regulate the genes that control metabolism throughout the body.
Is liothyronine FDA-approved?
Yes. Liothyronine is an FDA-approved medication with decades of clinical experience for the treatment of hypothyroidism and other thyroid conditions.
What does the research say about liothyronine?
Much of the active research concerns whether combined T4/T3 therapy benefits the subset of hypothyroid patients who report persistent symptoms despite normal TSH on levothyroxine alone. Results have been mixed, and sustained-release T3 formulations are being studied.
What are the safety concerns with liothyronine?
Side effects are largely predictable extensions of thyroid hormone action. At excessive doses, symptoms of thyrotoxicosis emerge, including rapid heartbeat, palpitations, tremor, anxiety, insomnia and weight loss. Cardiac effects are the most clinically important, particularly in older patients.
Research Handling & Storage
Reconstitution (General Guidelines)
Lyophilized peptides are typically reconstituted using bacteriostatic water (0.9% benzyl alcohol). Standard reconstitution protocol:
- Remove the vial from storage and allow it to reach room temperature (20–25°C / 68–77°F) before opening. This typically takes 15–20 minutes.
- Clean the vial stopper with an alcohol prep pad and allow to air dry.
- Using a sterile syringe, slowly inject bacteriostatic water along the inside wall of the vial. Do not spray directly onto the lyophilized powder.
- Gently swirl the vial until the powder is fully dissolved. Do not shake vigorously as this may damage the peptide structure.
- The reconstituted solution should be clear and colorless. Discard if cloudy, discolored, or if particulate matter is visible.
- Label the vial with the reconstitution date, concentration, and your initials.
Common reconstitution volumes in research: 1ml or 2ml of bacteriostatic water per vial, depending on the desired concentration. For example, adding 2ml to a 5mg vial yields a concentration of 2.5mg/ml (2,500mcg/ml).
Storage
- Lyophilized (unreconstituted): Store at -20°C (-4°F) for long-term storage (stable 24+ months), or 2–8°C (36–46°F) refrigerated for short-term storage up to 6 months. Keep desiccated and protected from light.
- Reconstituted: Store at 2–8°C (36–46°F) refrigerated. Use within 4–6 weeks of reconstitution. Do not freeze reconstituted solutions as this may cause degradation.
- Shipping: Lyophilized peptides are generally stable at ambient temperature during transit for several days. Reconstituted solutions should be shipped on ice packs.
Handling Precautions
- Handle with appropriate personal protective equipment (PPE) including nitrile gloves, lab coat, and eye protection.
- Use aseptic/sterile technique when reconstituting and transferring solutions to prevent contamination.
- Avoid repeated freeze-thaw cycles which may denature the compound and reduce potency.
- Keep detailed laboratory records including reconstitution dates, lot numbers, concentrations, and storage conditions.
- Dispose of unused material and sharps in accordance with local regulations and institutional biosafety guidelines.
Stability & Shelf Life
Lyophilized (freeze-dried) peptides are highly stable when stored correctly. At -20°C (-4°F), most peptides retain >95% purity for 24 months or longer. Once reconstituted, the clock starts—proteins in solution are inherently less stable than in dry form. Factors that accelerate degradation include temperature fluctuations, exposure to light, repeated freeze-thaw cycles, bacterial contamination, and oxidation.
Purity & Quality Considerations
Research-grade compounds should be accompanied by a Certificate of Analysis (COA) confirming purity, typically verified by High-Performance Liquid Chromatography (HPLC) and Mass Spectrometry (MS). Look for purity levels of ≥98% for research applications. Third-party testing adds an additional layer of quality assurance. Always verify the source and documentation before using any research compound.
Research Supplies & Resources
Essential supplies and educational resources for peptide research. Links go to Amazon.com.
Lab Supplies
Recommended Reading
Lab Equipment
As an Amazon Associate, peptides.fyi earns from qualifying purchases. Learn more.