Synopsis
Compound overview
- Research only
- In clinical trials
- Approved outside US
- FDA-approved
What it is
S-4 (andarine) is one of the earlier selective androgen receptor modulators (SARMs). It never advanced through clinical development and is sold only as a research chemical.
What it does
How it has been studied and marketed:
- Studied for muscle and bone effects in early research
- Promoted (illegally) as a "legal steroid" alternative
- Known for a distinctive vision side effect
- Banned in all competitive sport
How it works
S-4 binds androgen receptors in muscle and bone tissue. It also binds receptors in the eye, which is thought to cause its well-known visual side effects.
Safety notes
S-4 is not approved for human use. Users commonly report a yellow tint to vision and trouble seeing in low light, alongside the testosterone suppression and cholesterol changes seen with other SARMs. The FDA has warned against SARMs, and research-grade purity varies widely.
Where to buy S4 (Andarine)
Standard lyophilized vial — reconstitute and measure doses yourself. The conventional research format.
Affiliate links — we may earn a commission at no extra cost to you.
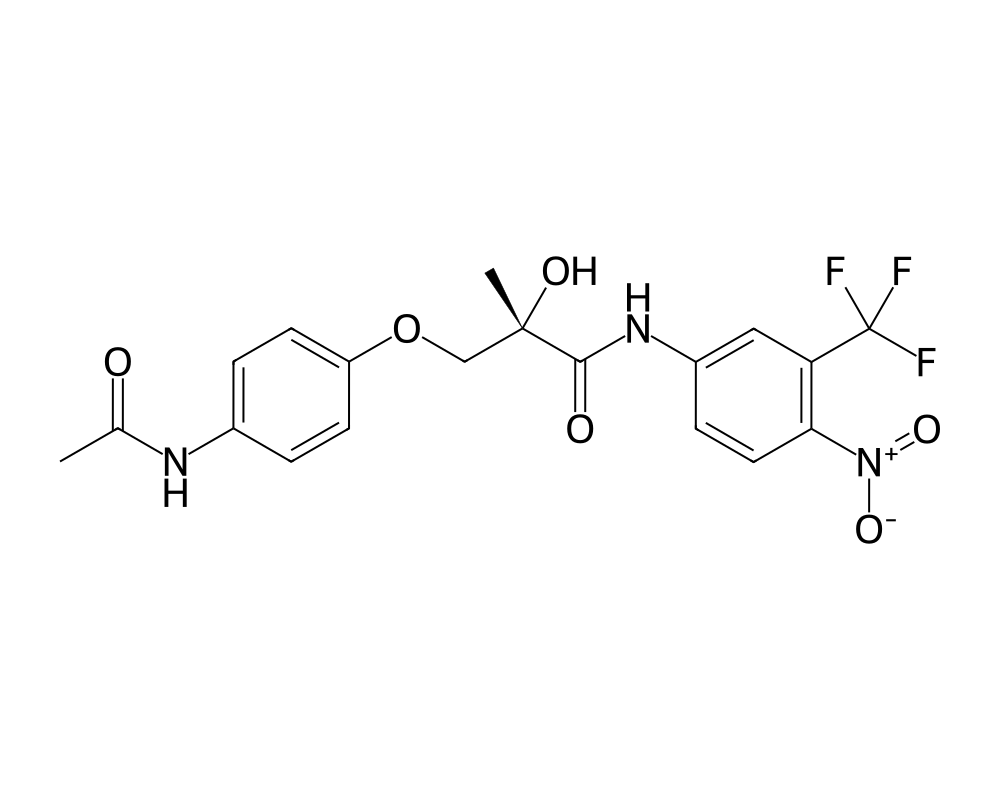
Molecular Structure
Research tool
Reconstitution calculator
Concentration
2.50mg/mL
Draw volume
0.10mL
Insulin units
10IU
Doses/vial
20
Overview
S4, also known as Andarine or GTx-007, is a non-steroidal selective androgen receptor modulator developed by GTx, Inc. as part of the same research program that produced Ostarine (MK-2866). Andarine was among the first SARMs to be characterized in preclinical studies and played an important role in establishing the proof of concept for tissue-selective androgen receptor modulation. While it was eventually superseded in GTx’s clinical development pipeline by Ostarine, Andarine remains a scientifically significant compound with a substantial preclinical evidence base.
Contents
The compound emerged from a medicinal chemistry campaign that screened thousands of non-steroidal AR ligands for anabolic activity in muscle and bone with minimal stimulation of the prostate. Andarine showed promising tissue selectivity in early animal studies, maintaining approximately 30% to 40% of the anabolic activity of testosterone propionate in the levator ani muscle while producing less than 10% of testosterone’s prostate stimulation. This separation ratio, while not as dramatic as some later SARMs, was sufficient to establish the pharmacological viability of the SARM concept.
Mechanism of Action
Andarine binds to the androgen receptor as a partial agonist. This is a critical distinction from full agonists like testosterone and from other SARMs that approach full agonist efficacy in muscle tissue. As a partial agonist, Andarine produces submaximal receptor activation even at saturating concentrations. In tissues where androgen receptor density is high and full activation is the normal physiological state (such as the prostate), partial agonism means Andarine cannot match the stimulatory effects of endogenous androgens. In muscle, where partial agonism may still be sufficient to drive meaningful anabolic transcription, the compound can produce disproportionate benefit.
The partial agonist profile also means that Andarine can function as a competitive antagonist in the presence of high endogenous androgen levels. By occupying AR binding sites without fully activating them, the compound can effectively reduce androgenic stimulation of target tissues. This property has been explored in preclinical models of benign prostatic hyperplasia (BPH), where Andarine reduced prostate weight without eliminating androgen signaling entirely.
Andarine’s pharmacokinetics in animal models show rapid oral absorption, with peak plasma concentrations reached within one to two hours. The half-life is relatively short, approximately four to six hours in rats, which has implications for dosing frequency. Metabolism occurs through oxidative and conjugative pathways, with several metabolites identified in preclinical species.
Research Summary
The preclinical evidence base for Andarine includes several important studies. In castrated male rats, Andarine restored levator ani muscle weight to near-sham levels while producing only modest increases in prostate and seminal vesicle weight. This tissue-selective profile was maintained across a range of doses, establishing the compound as a true SARM in the pharmacological sense.
In ovariectomized female rats (a model of postmenopausal bone loss), Andarine prevented bone mineral density loss and maintained bone strength as effectively as DHT, without producing the virilizing effects of the androgen. This finding supported the potential utility of SARMs in osteoporosis, a therapeutic area where the anabolic effects of androgens are desired but the masculinizing effects are unacceptable.
Studies in intact male rats demonstrated that Andarine could reduce prostate weight when administered at doses that maintained muscle mass, consistent with its partial agonist profile. This observation led to research exploring Andarine as a potential treatment for BPH, where the goal is to reduce prostate size while preserving lean mass and physical function.
Despite these promising preclinical results, GTx chose to advance Ostarine rather than Andarine into clinical trials, reportedly due to Ostarine’s superior tissue selectivity and more favorable pharmacokinetic profile. No human clinical trial data for Andarine have been published, though the compound has been detected in anti-doping analyses of athlete samples, confirming that it is used in non-clinical contexts.
Dosing in Published Research
About this section
The information below reports dosing only as it appears in published clinical or preclinical research and official regulatory documents. It is provided as published-literature reference material. It is not dosing guidance, not medical advice, and not a recommendation to use or self-administer this compound.
S4 (andarine) is a selective androgen receptor modulator. It has not been the subject of published human clinical trials, so no controlled study has established a dose for it in people. Specific S4 figures circulating in forums or vendor material are not derived from human research and are therefore not reported here.
No established human dosing
Because no human trial has established a dose for S4, any specific figures circulating online are unverified. S4 is not an approved drug, is prohibited in sport by WADA, and material sold under this name is for laboratory research use only.
Safety and Side Effects
The most widely discussed side effect associated with Andarine is a visual disturbance described as a yellow tint to vision and difficulty adapting to changes in light conditions, particularly at night. This effect has been attributed to Andarine’s binding to retinal receptors, though the precise molecular target has not been definitively identified. Some researchers have proposed that the compound or a metabolite interacts with the retinal photoreceptor system, possibly through off-target binding to retinal androgen receptors or a distinct receptor in the visual pathway.
The visual side effect appears to be dose-dependent and reversible upon discontinuation. Reports from the research community suggest it is most prominent at doses exceeding 50 mg daily and resolves within one to two weeks of stopping administration. No permanent visual damage has been reported, though the absence of formal ophthalmological studies means that subclinical effects on retinal function cannot be excluded.
Hormonal suppression is expected based on Andarine’s AR agonist activity. User reports describe dose-dependent testosterone suppression, with recovery generally occurring within four to six weeks of discontinuation. HDL cholesterol reductions have been reported at doses commonly used in the research community (25 to 75 mg daily).
No formal toxicology studies have been published, and the safety of Andarine in humans has not been evaluated through regulatory processes. Hepatotoxicity data are unavailable from controlled studies, though user-reported bloodwork has not consistently shown liver enzyme elevations at commonly used doses.
Current Research Status
Andarine is an investigational compound that was not advanced to clinical trials by its developer. It has no approved medical indications and is prohibited by WADA. The compound remains available through research chemical suppliers and continues to be studied in academic laboratories investigating SARM pharmacology, androgen receptor biology, and tissue-selective androgen signaling. Its historical importance as one of the first well-characterized non-steroidal SARMs ensures its continued relevance in the scientific literature, even as newer compounds with potentially superior profiles have emerged.
Further reading: For a comparison of two related selective androgen receptor modulators, see RAD-140 vs LGD-4033: Comparing Two Researched SARMs.
Frequently Asked Questions
What is S4 (Andarine)?
S4, also known as Andarine, is one of the earlier non-steroidal selective androgen receptor modulators (SARMs), developed by GTx, Inc. It never advanced through clinical development and is sold only as a research chemical.
How does S4 (Andarine) work?
Andarine binds the androgen receptor as a partial agonist, producing submaximal receptor activation even at high concentrations. In animal studies this gave a tissue-selective profile favoring muscle and bone over prostate tissue.
Is S4 (Andarine) FDA-approved?
No. Andarine is an investigational compound that was not advanced to clinical trials by its developer. It has no approved medical indications and is prohibited by WADA.
What does the research say about S4 (Andarine)?
The evidence base is preclinical. In castrated male rats, Andarine restored muscle weight with only modest effects on prostate tissue, showing tissue selectivity. No human efficacy trials have been published.
What are the safety concerns with S4 (Andarine)?
The most widely discussed side effect is a visual disturbance described as a yellow tint to vision and difficulty adapting to light, attributed to binding at retinal receptors. Because the compound was never studied in humans, its broader safety profile is not characterized.
Research Handling & Storage
Reconstitution (General Guidelines)
Lyophilized peptides are typically reconstituted using bacteriostatic water (0.9% benzyl alcohol). Standard reconstitution protocol:
- Remove the vial from storage and allow it to reach room temperature (20–25°C / 68–77°F) before opening. This typically takes 15–20 minutes.
- Clean the vial stopper with an alcohol prep pad and allow to air dry.
- Using a sterile syringe, slowly inject bacteriostatic water along the inside wall of the vial. Do not spray directly onto the lyophilized powder.
- Gently swirl the vial until the powder is fully dissolved. Do not shake vigorously as this may damage the peptide structure.
- The reconstituted solution should be clear and colorless. Discard if cloudy, discolored, or if particulate matter is visible.
- Label the vial with the reconstitution date, concentration, and your initials.
Common reconstitution volumes in research: 1ml or 2ml of bacteriostatic water per vial, depending on the desired concentration. For example, adding 2ml to a 5mg vial yields a concentration of 2.5mg/ml (2,500mcg/ml).
Storage
- Lyophilized (unreconstituted): Store at -20°C (-4°F) for long-term storage (stable 24+ months), or 2–8°C (36–46°F) refrigerated for short-term storage up to 6 months. Keep desiccated and protected from light.
- Reconstituted: Store at 2–8°C (36–46°F) refrigerated. Use within 4–6 weeks of reconstitution. Do not freeze reconstituted solutions as this may cause degradation.
- Shipping: Lyophilized peptides are generally stable at ambient temperature during transit for several days. Reconstituted solutions should be shipped on ice packs.
Handling Precautions
- Handle with appropriate personal protective equipment (PPE) including nitrile gloves, lab coat, and eye protection.
- Use aseptic/sterile technique when reconstituting and transferring solutions to prevent contamination.
- Avoid repeated freeze-thaw cycles which may denature the compound and reduce potency.
- Keep detailed laboratory records including reconstitution dates, lot numbers, concentrations, and storage conditions.
- Dispose of unused material and sharps in accordance with local regulations and institutional biosafety guidelines.
Stability & Shelf Life
Lyophilized (freeze-dried) peptides are highly stable when stored correctly. At -20°C (-4°F), most peptides retain >95% purity for 24 months or longer. Once reconstituted, the clock starts—proteins in solution are inherently less stable than in dry form. Factors that accelerate degradation include temperature fluctuations, exposure to light, repeated freeze-thaw cycles, bacterial contamination, and oxidation.
Purity & Quality Considerations
Research-grade compounds should be accompanied by a Certificate of Analysis (COA) confirming purity, typically verified by High-Performance Liquid Chromatography (HPLC) and Mass Spectrometry (MS). Look for purity levels of ≥98% for research applications. Third-party testing adds an additional layer of quality assurance. Always verify the source and documentation before using any research compound.
Research Supplies & Resources
Essential supplies and educational resources for peptide research. Links go to Amazon.com.
Lab Supplies
Recommended Reading
Lab Equipment
As an Amazon Associate, peptides.fyi earns from qualifying purchases. Learn more.