Synopsis
Compound overview
- Research only
- In clinical trials
- Approved outside US
- FDA-approved
What it is
Sildenafil is a PDE5 inhibitor. It is an FDA-approved prescription medicine, best known as Viagra for erectile dysfunction and also sold as Revatio for a lung blood-pressure condition.
What it does
Documented clinical uses include:
- Treats erectile dysfunction
- Treats pulmonary arterial hypertension
- Acts faster but for a shorter time than tadalafil
- Has decades of clinical data
How it works
Sildenafil blocks PDE5, the enzyme that breaks down cGMP — the molecule that keeps blood vessels relaxed. The result is improved blood flow where the drug acts.
Safety notes
Sildenafil is prescription-only. It must not be combined with nitrate heart medicines because of the risk of a severe blood-pressure drop. Side effects include headache, flushing, indigestion and visual changes. Research-vendor material is not pharmacy-grade.
Where to buy Sildenafil
Standard lyophilized vial — reconstitute and measure doses yourself. The conventional research format.
Affiliate links — we may earn a commission at no extra cost to you.
Molecular Structure
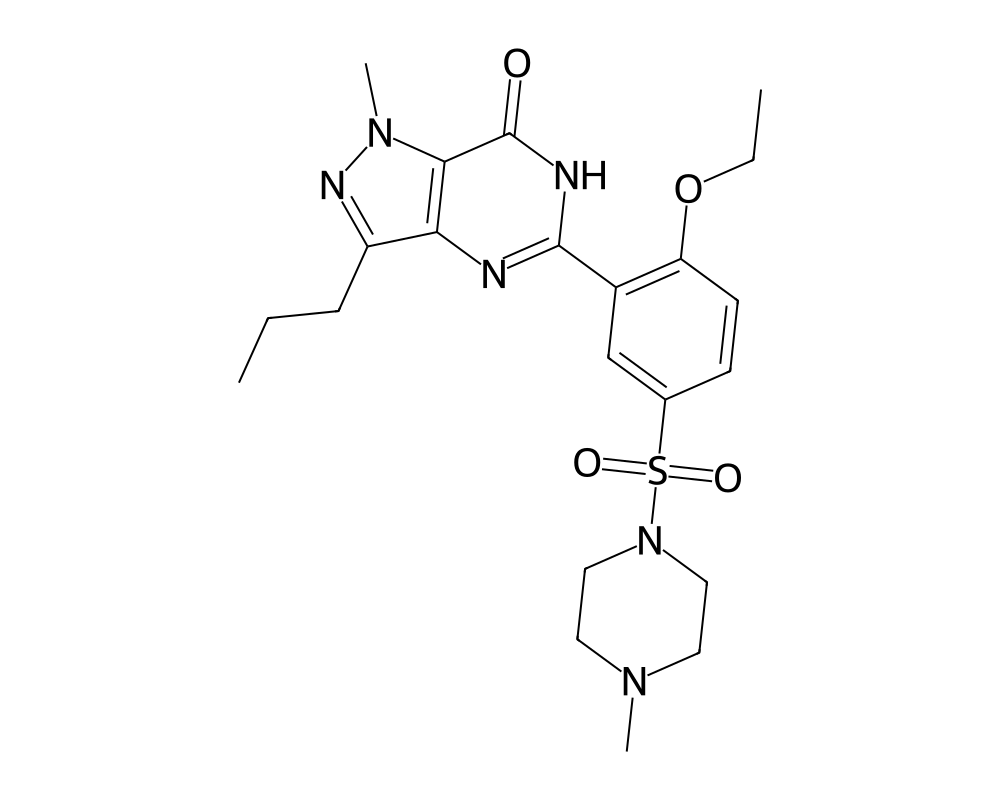
Overview
Sildenafil is a phosphodiesterase type 5 (PDE5) inhibitor developed by Pfizer scientists in the early 1990s. Originally investigated as a treatment for angina pectoris and hypertension, the compound famously pivoted to erectile dysfunction after clinical trial participants reported marked improvements in sexual function. Marketed as Viagra, it received FDA approval in 1998 and became one of the fastest-selling pharmaceutical products in history. A second indication, pulmonary arterial hypertension, was approved in 2005 under the brand name Revatio.
Contents
The story of sildenafil is frequently cited as a case study in serendipitous drug discovery. The Pfizer team, led by chemists Simon Campbell and David Roberts, synthesized the compound to target PDE5 in vascular smooth muscle, aiming to treat coronary artery disease. When the angina trials showed modest cardiovascular benefit but consistent reports of penile erection as a side effect, the investigators recognized the therapeutic opportunity and redirected development. That pivot transformed both the pharmaceutical industry and the cultural landscape surrounding sexual health.
Beyond its blockbuster commercial applications, sildenafil has become a valuable research tool for studying nitric oxide signaling, cyclic nucleotide physiology, and vascular biology. Its well-characterized mechanism and extensive safety database make it a reference compound in PDE5 inhibitor pharmacology.
Mechanism of Action
Sildenafil works by selectively inhibiting phosphodiesterase type 5, the enzyme primarily responsible for degrading cyclic guanosine monophosphate (cGMP) in the smooth muscle cells of the corpus cavernosum and pulmonary vasculature. Under normal physiological conditions, sexual stimulation triggers the release of nitric oxide (NO) from endothelial cells and nonadrenergic, noncholinergic nerve terminals in the penis. NO activates soluble guanylate cyclase, which catalyzes the production of cGMP from GTP.
cGMP acts as a second messenger, activating protein kinase G (PKG), which phosphorylates multiple downstream targets to produce smooth muscle relaxation. This relaxation allows blood to fill the sinusoidal spaces of the corpus cavernosum, producing an erection. PDE5 normally terminates this signaling cascade by hydrolyzing cGMP back to inactive 5′-GMP. By blocking PDE5, sildenafil prolongs and amplifies the cGMP signal, enhancing the erectile response to sexual stimulation.
Importantly, sildenafil does not initiate erection independently. It requires upstream NO release, which depends on sexual arousal. This pharmacological characteristic distinguishes PDE5 inhibitors from direct-acting vasodilators and explains why the compound does not cause persistent unwanted erections under normal circumstances.
In the pulmonary vasculature, the same mechanism produces vasorelaxation of pulmonary arterial smooth muscle, reducing pulmonary vascular resistance and improving exercise capacity in patients with pulmonary arterial hypertension. PDE5 is expressed at particularly high levels in pulmonary tissue, which provides a degree of tissue selectivity for this indication.
Research Summary
The clinical evidence supporting sildenafil for erectile dysfunction is vast. The pivotal trials demonstrated efficacy across a range of etiologies, including psychogenic, organic, and mixed erectile dysfunction. Response rates (defined as improved erections sufficient for intercourse) ranged from 56% to 84% depending on the study population, with higher response rates in psychogenic and mild organic ED and lower rates in severe organic ED, particularly in patients with diabetes or radical prostatectomy.
For pulmonary arterial hypertension, the SUPER-1 trial demonstrated that sildenafil at 20 mg three times daily improved exercise capacity (measured by six-minute walk distance), reduced mean pulmonary artery pressure, and improved WHO functional class in patients with PAH. Long-term extension studies showed sustained benefit over periods exceeding three years.
Research has expanded into numerous additional areas. Studies have investigated sildenafil for Raynaud’s phenomenon, altitude sickness, heart failure with preserved ejection fraction, female sexual dysfunction, lymphatic malformations, and even as a neuroprotective agent. In preclinical models, PDE5 inhibition has shown cardioprotective effects during ischemia-reperfusion injury, anti-fibrotic properties, and anti-apoptotic actions in neuronal tissue.
Pharmacokinetic studies show rapid oral absorption, with peak plasma concentrations reached within 30 to 120 minutes. The terminal half-life is approximately four hours, though clinical effect duration extends somewhat longer. High-fat meals delay absorption significantly. Metabolism occurs primarily through CYP3A4, with CYP2C9 playing a minor role, generating the active metabolite N-desmethyl sildenafil.
Dosing in Published Research
About this section
The information below reports dosing only as it appears in published clinical or preclinical research and official regulatory documents. It is provided as published-literature reference material. It is not dosing guidance, not medical advice, and not a recommendation to use or self-administer this compound.
Sildenafil is an FDA-approved prescription medicine, so its dosing is defined by approved product labeling. The FDA-approved labeling describes:
- Erectile dysfunction (Viagra): a 50 mg dose taken about one hour before sexual activity, within a window of roughly 30 minutes to 4 hours beforehand; adjustable to 100 mg or down to 25 mg, with a maximum of one dose per day. A 25 mg starting dose is suggested for certain patients.
- Pulmonary arterial hypertension (Revatio): 20 mg three times daily.
These figures are drawn from FDA-approved prescribing information.
Important
Sildenafil can cause a dangerous, potentially fatal drop in blood pressure when combined with nitrate medications. The doses above describe the approved prescription product used under medical supervision; they are not a recommendation, and they do not apply to material sold for laboratory or research use, which is not the approved drug product.
Safety and Side Effects
The safety profile of sildenafil has been extensively characterized through clinical trials involving tens of thousands of subjects and post-marketing surveillance spanning more than two decades. The most common adverse effects reflect PDE5 inhibition in non-target vascular beds: headache (occurring in 16% to 28% of subjects), facial flushing (10% to 19%), dyspepsia (7% to 17%), and nasal congestion (4% to 9%). These effects are generally mild, dose-dependent, and self-limiting.
Visual disturbances, including a blue-green color tinge to vision and increased light sensitivity, occur in a minority of users and result from weak inhibition of PDE6 in retinal photoreceptors. Rare cases of non-arteritic anterior ischemic optic neuropathy (NAION) have been reported, though a causal relationship has not been definitively established.
The most critical safety concern involves the co-administration of sildenafil with organic nitrates or nitric oxide donors. Both agents increase cGMP levels through different mechanisms, and their combination can produce severe, potentially fatal hypotension. This interaction is an absolute contraindication and represents the most important prescribing consideration for the compound.
Cardiovascular safety in patients with stable coronary artery disease has been reassuring. Multiple studies and the Princeton III Consensus Conference have concluded that PDE5 inhibitors are safe in patients who can tolerate the physical exertion equivalent to sexual activity (generally four to six metabolic equivalents) and who are not taking nitrates. Sildenafil has no clinically significant effect on cardiac contractility, conduction, or repolarization at standard doses.
Priapism (prolonged erection exceeding four hours) is a rare but serious potential complication requiring emergency medical intervention. Patients with conditions predisposing to priapism, including sickle cell disease, multiple myeloma, and leukemia, face elevated risk.
Current Research Status
Sildenafil is FDA-approved for erectile dysfunction and pulmonary arterial hypertension, with generic formulations widely available since the original patent expiration in 2020. Active research areas include its potential role in heart failure management, neuroprotection following stroke and traumatic brain injury, cancer biology (where PDE5 inhibition may modulate tumor immune evasion), and fetal growth restriction in complicated pregnancies. The compound’s well-understood mechanism and extensive safety record continue to make it a starting point for investigations into cGMP-mediated physiology across diverse organ systems.
Frequently Asked Questions
What is sildenafil?
Sildenafil is a PDE5 inhibitor and an FDA-approved prescription medicine. It is best known as Viagra for erectile dysfunction and is also sold as Revatio for pulmonary arterial hypertension.
How does sildenafil work?
Sildenafil blocks PDE5, the enzyme that breaks down cGMP, the molecule that keeps blood vessels relaxed. With PDE5 inhibited, cGMP levels rise, allowing smooth muscle to relax and blood flow to increase in response to stimulation.
Is sildenafil FDA-approved?
Yes. Sildenafil is FDA-approved for erectile dysfunction and pulmonary arterial hypertension, and generic versions have been widely available since the original patent expired in 2020.
What does the research say about sildenafil?
The clinical evidence for erectile dysfunction is vast, with pivotal trials showing efficacy across psychogenic, organic and mixed causes. It has decades of clinical data, and acts faster but for a shorter duration than tadalafil.
What are the safety concerns with sildenafil?
Sildenafil’s safety has been characterized through trials in tens of thousands of subjects and over two decades of post-marketing use. The most common side effects reflect PDE5 inhibition in non-target blood vessels, including headache, flushing and nasal congestion. It can interact dangerously with nitrate medications.
Research Handling & Storage
Storage
- Unopened: Store at controlled room temperature, 20–25°C (68–77°F), away from direct sunlight, heat, and moisture.
- Opened: Keep container tightly closed. Use within the timeframe indicated on the label, typically 30–90 days after opening.
- Do not freeze liquid solutions unless specifically indicated.
Handling Precautions
- Handle with appropriate personal protective equipment (PPE) including nitrile gloves, lab coat, and eye protection.
- Use aseptic/sterile technique when reconstituting and transferring solutions to prevent contamination.
- Avoid repeated freeze-thaw cycles which may denature the compound and reduce potency.
- Keep detailed laboratory records including reconstitution dates, lot numbers, concentrations, and storage conditions.
- Dispose of unused material and sharps in accordance with local regulations and institutional biosafety guidelines.
Stability & Shelf Life
Liquid formulations typically remain stable for 1–2 years when stored at the recommended temperature in the original sealed container. Once opened, potency may gradually decrease. Monitor for any changes in color, clarity, or odor, which may indicate degradation.
Purity & Quality Considerations
Research-grade compounds should be accompanied by a Certificate of Analysis (COA) confirming purity, typically verified by High-Performance Liquid Chromatography (HPLC) and Mass Spectrometry (MS). Look for purity levels of ≥98% for research applications. Third-party testing adds an additional layer of quality assurance. Always verify the source and documentation before using any research compound.
Research Supplies & Resources
Essential supplies and educational resources for peptide research. Links go to Amazon.com.
Lab Supplies
Recommended Reading
Lab Equipment
As an Amazon Associate, peptides.fyi earns from qualifying purchases. Learn more.