Synopsis
Compound overview
- Research only
- In clinical trials
- Approved outside US
- FDA-approved
What it is
Thymosin alpha-1 (thymalfasin) is a synthetic copy of a natural immune-system peptide made by the thymus gland. It is approved as a medicine in a number of countries — sold as Zadaxin — but it is not FDA-approved in the US.
What it does
Documented and studied uses include:
- Used abroad to treat hepatitis B
- Studied as an immune-system modulator
- Researched alongside some cancer treatments
- Investigated in infectious-disease research
How it works
Thymosin alpha-1 helps regulate the immune system, particularly the maturation and activity of T-cells, which are central to fighting infections.
Safety notes
Thymosin alpha-1 is approved only outside the US, and uses there are specific and medically supervised. As a research chemical it has no FDA review behind it, immune-modulating compounds can have unpredictable effects, and research-grade purity varies.
Where to buy Thymosin Alpha-1
Standard lyophilized vial — reconstitute and measure doses yourself. The conventional research format.
Affiliate links — we may earn a commission at no extra cost to you.
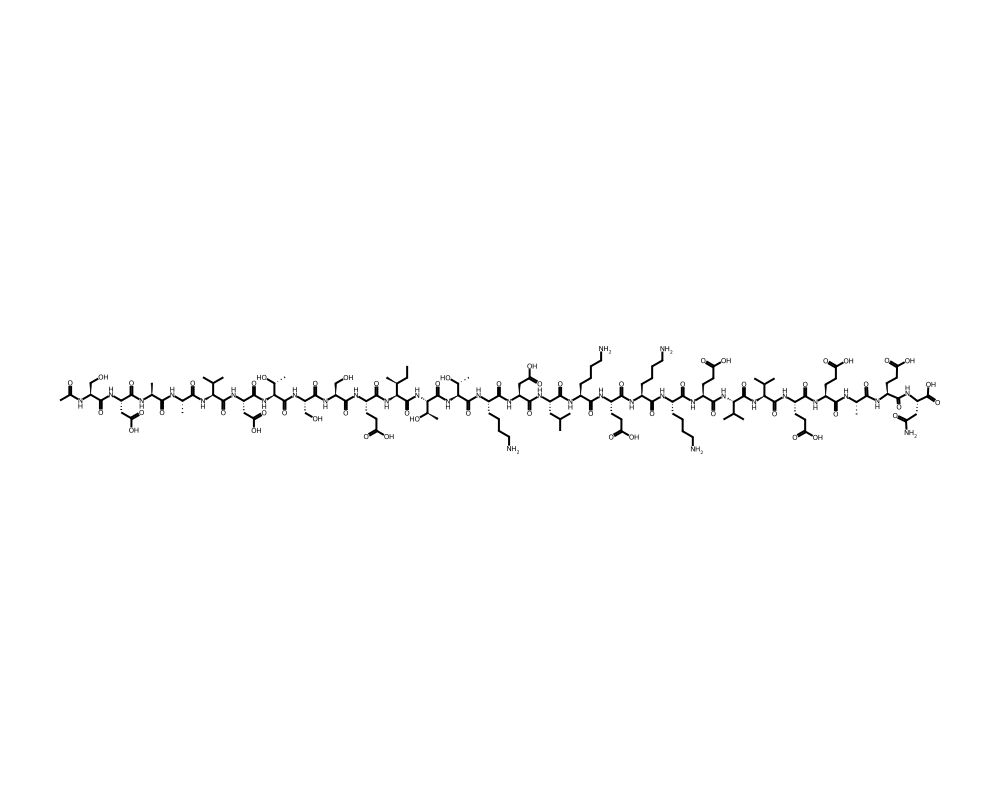
Molecular Structure
Research tool
Reconstitution calculator
Concentration
2.50mg/mL
Draw volume
0.10mL
Insulin units
10IU
Doses/vial
20
Overview
Thymosin alpha-1 (Ta1) is a 28-amino acid peptide originally isolated from thymic tissue by Allan Goldstein and colleagues at George Washington University in 1977. The thymus gland, a lymphoid organ located behind the sternum, plays a critical role in the maturation and education of T lymphocytes, the adaptive immune cells responsible for defending against infections and cancer. Thymosin alpha-1 was identified as one of the key bioactive components of “thymosin fraction 5,” a partially purified extract of calf thymus tissue that had shown immunostimulatory properties in early immunological research.
Contents
The peptide has had a notable, if geographically uneven, clinical history. While thymosin alpha-1 has never been approved by the FDA, it is approved in over 35 countries, primarily in Asia, South America, and Eastern Europe, where it is marketed under the trade name Zadaxin (manufactured by SciClone Pharmaceuticals). Its approved indications vary by country but include chronic hepatitis B, chronic hepatitis C (as an adjunct to interferon), and as an immune enhancer in immunocompromised patients.
Thymosin alpha-1 occupies an interesting niche in immunopharmacology. It is neither an immunosuppressant nor a simple immune stimulant. Instead, it functions as an immunomodulator that tends to normalize immune responses, boosting insufficient immunity while not exacerbating autoimmune or hyperinflammatory conditions. This regulatory quality, rather than a brute-force stimulatory effect, is what has made it attractive for clinical applications ranging from infectious disease to cancer immunotherapy to vaccine enhancement.
Mechanism of Action
Thymosin alpha-1 exerts its immunomodulatory effects through multiple interconnected mechanisms. Its primary targets are dendritic cells and T lymphocytes, the central players in adaptive immunity.
In dendritic cells, thymosin alpha-1 activates Toll-like receptor 9 (TLR9) and Toll-like receptor 2 (TLR2), which are pattern recognition receptors of the innate immune system. This activation promotes dendritic cell maturation, increases the expression of MHC class II molecules and co-stimulatory molecules (CD80, CD86), and enhances the production of cytokines including IL-12 and IFN-alpha. The net effect is improved antigen presentation and a stronger bridge between innate and adaptive immune responses.
On T lymphocytes, thymosin alpha-1 promotes the differentiation and maturation of T cell precursors, increases T cell receptor diversity, and enhances the functional capacity of mature T cells. It preferentially supports the development of Th1 (cell-mediated) immune responses, which are critical for defense against intracellular pathogens and tumor cells. Thymosin alpha-1 also increases the activity of natural killer (NK) cells and enhances antibody-dependent cellular cytotoxicity.
The peptide stimulates the expression of terminal deoxynucleotidyl transferase (TdT), an enzyme involved in generating T cell receptor diversity during T cell development in the thymus. By promoting TdT expression, thymosin alpha-1 may help maintain the diversity of the T cell repertoire, a function that naturally declines with age as the thymus involutes.
Thymosin alpha-1 also has anti-inflammatory properties, including the ability to suppress the production of pro-inflammatory cytokines such as TNF-alpha and IL-1 beta under conditions of excessive inflammation. This bidirectional regulatory capacity explains its classification as an immunomodulator rather than a simple immunostimulant.
Research Summary
The clinical research base for thymosin alpha-1 includes numerous controlled trials across several therapeutic areas.
In chronic hepatitis B, multiple randomized trials have demonstrated that thymosin alpha-1, administered as a course of twice-weekly subcutaneous injections over six months, produces sustained virological and biochemical responses in approximately 25 to 40 percent of patients. A meta-analysis published in the Journal of Viral Hepatitis confirmed that thymosin alpha-1 monotherapy significantly increased the rate of complete response compared to no treatment, and combination therapy with interferon-alpha produced higher response rates than either agent alone.
Hepatitis C research showed that thymosin alpha-1, when combined with interferon-alpha, improved sustained virological response rates compared to interferon alone, particularly in genotype 1 patients who are traditionally more difficult to treat. However, the advent of direct-acting antiviral agents for hepatitis C has largely superseded interferon-based regimens, reducing the current clinical relevance of these findings.
Cancer immunotherapy represents a growing area of thymosin alpha-1 research. Studies in hepatocellular carcinoma, melanoma, and non-small cell lung cancer have explored thymosin alpha-1 as an adjunct to chemotherapy, radiation, or other immunotherapies. In hepatocellular carcinoma patients treated with transcatheter arterial chemoembolization (TACE), post-procedural thymosin alpha-1 administration improved survival and reduced recurrence rates in several controlled trials.
Vaccine adjuvant research has shown that thymosin alpha-1 can enhance the immune response to influenza, hepatitis B, and other vaccines, particularly in elderly or immunocompromised populations who typically mount suboptimal vaccine responses. This application has attracted renewed attention in the context of pandemic preparedness.
During the COVID-19 pandemic, thymosin alpha-1 was used in China and other countries as an immune support therapy for hospitalized patients. Retrospective studies reported improved lymphocyte counts and clinical outcomes in patients who received thymosin alpha-1, though the absence of large randomized trials limits the strength of these conclusions.
Dosing in Published Research
About this section
The information below reports dosing only as it appears in published clinical or preclinical research and official regulatory documents. It is provided as published-literature reference material. It is not dosing guidance, not medical advice, and not a recommendation to use or self-administer this compound.
Thymosin alpha-1 is an immune-modulating peptide. It is not FDA-approved in the United States, but it is approved in many other countries (sold as Zadaxin, with the generic name thymalfasin), chiefly for chronic hepatitis B and as an immune adjuvant. Across multiple Phase III chronic hepatitis B trials, the dose studied was 1.6 mg given by subcutaneous injection twice weekly, over treatment courses of roughly 6 to 12 months. These figures describe what was administered in those trials and in the approved hepatitis labeling outside the US.
Research doses, not a protocol
The 1.6 mg twice-weekly figure was studied for hepatitis under medical supervision; it is not an established dose for the general wellness or longevity uses often discussed online, for which controlled evidence is limited. Thymosin alpha-1 is not FDA-approved, and material sold for research use is not a regulated drug product.
Safety and Side Effects
Thymosin alpha-1 has an excellent safety profile supported by decades of clinical use across millions of patient-treatments worldwide. The most commonly reported side effect is injection site discomfort (redness, pain, or swelling), which is mild and self-limiting. Systemic side effects are rare and typically limited to transient flu-like symptoms (low-grade fever, myalgia) that resolve within 24 hours.
Notably, thymosin alpha-1 has not been associated with the autoimmune complications that represent a concern with many immune-stimulating agents. This is attributed to its modulatory rather than purely stimulatory mechanism of action. Patients with autoimmune conditions have received thymosin alpha-1 in clinical settings without reported exacerbation of their underlying disease, though systematic data in this population are limited.
No dose-limiting toxicities have been identified in clinical trials, and the therapeutic index is considered wide. Drug interaction data are limited, but no significant interactions have been identified in the context of combination therapy with interferons, antivirals, or chemotherapeutic agents.
Current Research Status
Thymosin alpha-1 is approved in over 35 countries but not in the United States or European Union, where it retains orphan drug status for certain indications. Current research focuses on its role in cancer immunotherapy combinations (particularly with checkpoint inhibitors), vaccine enhancement for elderly and immunocompromised populations, and immune reconstitution in severe infectious diseases. The peptide is available through international pharmaceutical channels and compounding pharmacies. The COVID-19 pandemic reignited interest in thymosin alpha-1 as an immune support agent, and several clinical trials investigating its role in viral infections are ongoing or recently completed.
Frequently Asked Questions
What is thymosin alpha-1?
Thymosin alpha-1 (thymalfasin) is a synthetic copy of a natural 28-amino-acid immune peptide made by the thymus gland. It is approved as a medicine in a number of countries, sold as Zadaxin, but it is not FDA-approved in the United States.
How does thymosin alpha-1 work?
Thymosin alpha-1 helps regulate the immune system, acting mainly on dendritic cells and T lymphocytes. It activates Toll-like receptors on dendritic cells and supports the maturation and function of T cells in adaptive immunity.
Is thymosin alpha-1 FDA-approved?
No. Thymosin alpha-1 is approved in over 35 countries but not in the United States or the European Union, where it retains orphan drug status for certain indications.
What does the research say about thymosin alpha-1?
The clinical research base includes numerous controlled trials. In chronic hepatitis B, multiple randomized trials of a six-month course of twice-weekly injections have reported benefit. It has also been studied in cancer immunotherapy combinations and infectious disease.
What are the safety concerns with thymosin alpha-1?
Thymosin alpha-1 has a strong safety profile supported by decades of clinical use across many patient-treatments worldwide. The most common side effect is mild, self-limiting injection-site discomfort, and systemic side effects are rare.
Research Handling & Storage
Reconstitution (General Guidelines)
Lyophilized peptides are typically reconstituted using bacteriostatic water (0.9% benzyl alcohol). Standard reconstitution protocol:
- Remove the vial from storage and allow it to reach room temperature (20–25°C / 68–77°F) before opening. This typically takes 15–20 minutes.
- Clean the vial stopper with an alcohol prep pad and allow to air dry.
- Using a sterile syringe, slowly inject bacteriostatic water along the inside wall of the vial. Do not spray directly onto the lyophilized powder.
- Gently swirl the vial until the powder is fully dissolved. Do not shake vigorously as this may damage the peptide structure.
- The reconstituted solution should be clear and colorless. Discard if cloudy, discolored, or if particulate matter is visible.
- Label the vial with the reconstitution date, concentration, and your initials.
Common reconstitution volumes in research: 1ml or 2ml of bacteriostatic water per vial, depending on the desired concentration. For example, adding 2ml to a 5mg vial yields a concentration of 2.5mg/ml (2,500mcg/ml).
Storage
- Lyophilized (unreconstituted): Store at -20°C (-4°F) for long-term storage (stable 24+ months), or 2–8°C (36–46°F) refrigerated for short-term storage up to 6 months. Keep desiccated and protected from light.
- Reconstituted: Store at 2–8°C (36–46°F) refrigerated. Use within 4–6 weeks of reconstitution. Do not freeze reconstituted solutions as this may cause degradation.
- Shipping: Lyophilized peptides are generally stable at ambient temperature during transit for several days. Reconstituted solutions should be shipped on ice packs.
Handling Precautions
- Handle with appropriate personal protective equipment (PPE) including nitrile gloves, lab coat, and eye protection.
- Use aseptic/sterile technique when reconstituting and transferring solutions to prevent contamination.
- Avoid repeated freeze-thaw cycles which may denature the compound and reduce potency.
- Keep detailed laboratory records including reconstitution dates, lot numbers, concentrations, and storage conditions.
- Dispose of unused material and sharps in accordance with local regulations and institutional biosafety guidelines.
Stability & Shelf Life
Lyophilized (freeze-dried) peptides are highly stable when stored correctly. At -20°C (-4°F), most peptides retain >95% purity for 24 months or longer. Once reconstituted, the clock starts—proteins in solution are inherently less stable than in dry form. Factors that accelerate degradation include temperature fluctuations, exposure to light, repeated freeze-thaw cycles, bacterial contamination, and oxidation.
Purity & Quality Considerations
Research-grade compounds should be accompanied by a Certificate of Analysis (COA) confirming purity, typically verified by High-Performance Liquid Chromatography (HPLC) and Mass Spectrometry (MS). Look for purity levels of ≥98% for research applications. Third-party testing adds an additional layer of quality assurance. Always verify the source and documentation before using any research compound.
Research Supplies & Resources
Essential supplies and educational resources for peptide research. Links go to Amazon.com.
Lab Supplies
Recommended Reading
Lab Equipment
As an Amazon Associate, peptides.fyi earns from qualifying purchases. Learn more.