Synopsis
Compound overview
- Research only
- In clinical trials
- Approved outside US
- FDA-approved
What it is
Oxytocin is a natural hormone made in the brain that plays a role in childbirth, bonding and social behaviour. A synthetic form is an FDA-approved medicine, used in hospitals (as Pitocin) mainly to induce or support labour.
What it does
Documented and studied roles include:
- Used medically to induce or strengthen labour
- Involved in milk release during breastfeeding
- Studied for roles in bonding and trust
- Researched in social and mood contexts
How it works
Oxytocin binds oxytocin receptors, causing the uterus to contract and milk ducts to release milk. In the brain it influences circuits tied to social bonding and stress.
Safety notes
Medical oxytocin is used in tightly controlled hospital settings because incorrect dosing during labour can be dangerous for mother and baby. Nasal or research-grade oxytocin sold for "bonding" or mood effects is not an approved use, and those products are unregulated.
Where to buy Oxytocin
Standard lyophilized vial — reconstitute and measure doses yourself. The conventional research format.
Affiliate links — we may earn a commission at no extra cost to you.
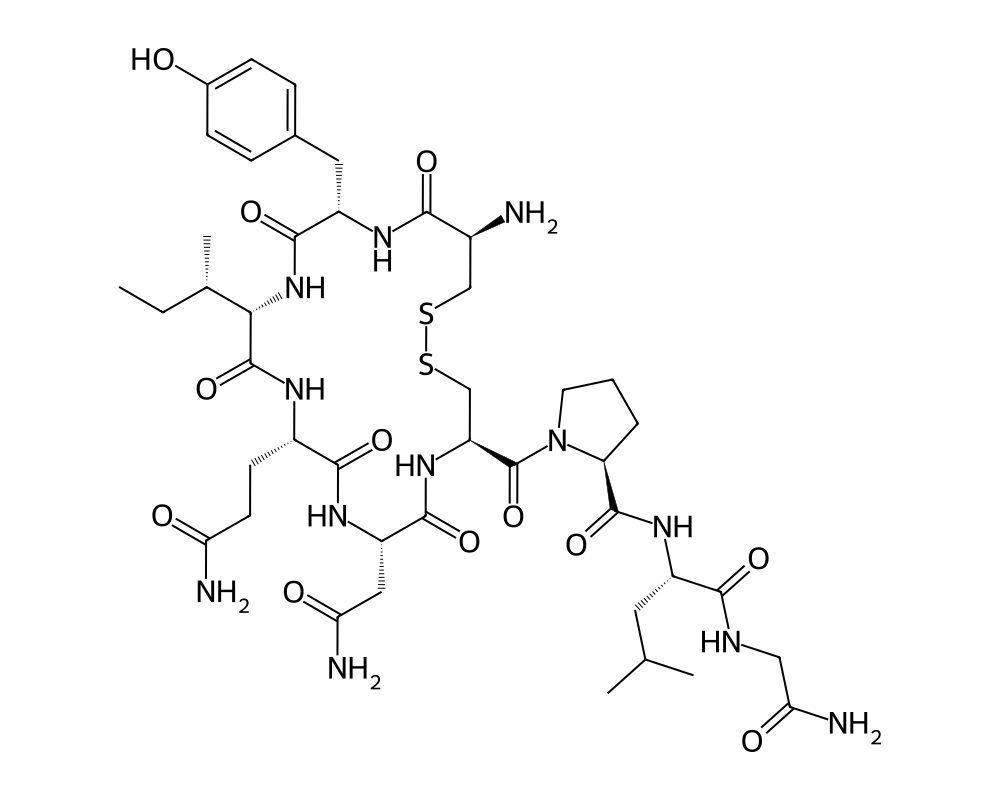
Molecular Structure
Research tool
Reconstitution calculator
Concentration
2.50mg/mL
Draw volume
0.10mL
Insulin units
10IU
Doses/vial
20
Overview
Oxytocin is a nine-amino acid cyclic peptide hormone produced primarily in the hypothalamus and released from the posterior pituitary gland. It is one of the oldest known peptide hormones, first isolated and synthesized by Vincent du Vigneaud in 1953, work that earned him the Nobel Prize in Chemistry in 1955. For most of the 20th century, oxytocin was understood primarily in the context of two functions: stimulating uterine contractions during labor and triggering milk letdown during breastfeeding. These remain its only FDA-approved clinical indications (marketed as Pitocin for labor induction).
Contents
The past three decades, however, have revealed an entirely different dimension of oxytocin biology. Beginning with landmark studies in prairie voles in the 1990s, researchers discovered that oxytocin plays a fundamental role in social bonding, trust, empathy, and emotional regulation. These findings transformed oxytocin from a peripheral reproductive hormone into one of the most studied molecules in social neuroscience, earning it the popular nickname “the love hormone” or “the bonding hormone,” though these labels substantially oversimplify its effects.
Oxytocin’s structure consists of a six-amino acid ring formed by a disulfide bridge between two cysteine residues, with a three-amino acid tail. This compact structure is closely related to vasopressin (antidiuretic hormone), which differs by only two amino acids. The structural similarity between these peptides has implications for their pharmacology, as oxytocin can bind to vasopressin receptors at high concentrations, and vice versa, complicating the interpretation of high-dose studies.
Mechanism of Action
Oxytocin acts through the oxytocin receptor (OXTR), a G-protein coupled receptor that signals primarily through the Gq/11 pathway, activating phospholipase C and increasing intracellular calcium. The oxytocin receptor is expressed widely throughout the body, including the uterus, mammary glands, brain, heart, kidneys, and immune cells. This broad distribution underlies the peptide’s diverse physiological effects.
In the brain, oxytocin modulates neurotransmission in regions critical for social behavior, emotional processing, and stress responses. Oxytocin neurons project from the paraventricular nucleus (PVN) and supraoptic nucleus (SON) of the hypothalamus to the amygdala, hippocampus, nucleus accumbens, and prefrontal cortex, among other regions. In the amygdala, oxytocin reduces the firing of neurons that respond to fear-inducing stimuli, which is thought to underlie its anxiolytic and trust-enhancing effects. In the nucleus accumbens, oxytocin interacts with dopaminergic reward circuitry, contributing to the rewarding nature of social interactions.
Oxytocin also has potent anti-inflammatory and immune-modulating effects. It reduces pro-inflammatory cytokine production, promotes wound healing, and modulates the activity of immune cells. In the cardiovascular system, oxytocin has direct vasodilatory and cardioprotective properties, reducing blood pressure and promoting cardiomyocyte differentiation.
An important pharmacological consideration is the blood-brain barrier (BBB). Peripherally administered oxytocin crosses the BBB poorly, and the extent to which intranasal administration (the most common route in behavioral research) delivers meaningful concentrations to the central nervous system remains debated. Some researchers have proposed that peripheral oxytocin effects on vagal afferents, rather than direct central penetration, may mediate some of the behavioral effects observed in intranasal studies.
Research Summary
The volume of oxytocin research is enormous, spanning reproductive biology, neuroscience, psychiatry, and cardiology. A comprehensive review is impossible in this format, but several key domains deserve attention.
Social behavior research has consistently shown that intranasal oxytocin increases trust in economic games, enhances the ability to read emotional expressions, promotes in-group favoritism, and reduces social anxiety. A seminal 2005 study in Nature demonstrated that intranasal oxytocin increased trusting behavior in a monetary investment game, a finding that launched a wave of research into oxytocin’s effects on social decision-making. However, subsequent research has revealed significant nuance: oxytocin’s effects on social behavior are context-dependent, and in some circumstances, it can increase out-group hostility, envy, or gloating, suggesting that it amplifies the salience of social information rather than simply promoting prosocial behavior.
Psychiatric research has explored intranasal oxytocin as a potential treatment for autism spectrum disorder (ASD), social anxiety disorder, schizophrenia, and post-traumatic stress disorder (PTSD). Results have been mixed. Early studies in ASD showed promising improvements in social cognition and eye contact, but larger, more rigorous trials have yielded inconsistent results. A 2021 meta-analysis concluded that the evidence for oxytocin’s efficacy in ASD is not yet sufficient to support clinical use.
Research on oxytocin’s metabolic effects has gained attention, with studies showing that intranasal oxytocin can reduce caloric intake and food-seeking behavior in both lean and obese subjects. This appetite-suppressing effect appears to be mediated by central mechanisms distinct from the peptide’s social effects.
Pain research has revealed that oxytocin has analgesic properties, likely mediated through both central and peripheral mechanisms. Clinical studies have reported reduced pain perception in chronic pain conditions, migraines, and experimental pain models following oxytocin administration.
Dosing in Published Research
About this section
The information below reports dosing only as it appears in published clinical or preclinical research and official regulatory documents. It is provided as published-literature reference material. It is not dosing guidance, not medical advice, and not a recommendation to use or self-administer this compound.
Oxytocin appears in the literature in two very different contexts:
- FDA-approved obstetric use (Pitocin): for induction or stimulation of labor, the FDA-approved labeling describes an intravenous infusion started at 0.5 to 1 milliunit per minute and increased gradually in 1 to 2 milliunit-per-minute increments every 30 to 60 minutes. This is given only in a hospital setting by clinicians.
- Intranasal oxytocin in behavioral research: this route is not FDA-approved. Across published human social-cognition studies, intranasal doses have ranged from roughly 10 to 72 international units per session, with 24 IU being the most commonly used single dose.
These figures are drawn from FDA-approved prescribing information and from the published intranasal-oxytocin research literature.
Important
Intranasal oxytocin has no FDA-approved use for behavioral, cognitive, or social purposes; the research doses above describe what investigators administered in controlled studies and are not a recommendation. The obstetric infusion regimen is a hospital procedure and does not apply to material sold for research use.
Safety and Side Effects
Intravenous oxytocin (Pitocin) for labor induction has a well-characterized safety profile backed by decades of obstetric use. Known risks include uterine hyperstimulation, fetal distress from excessive contractions, and (rarely) uterine rupture at high doses. These are dose-dependent effects directly related to the peptide’s contractile action on the uterus.
Intranasal oxytocin, as used in behavioral research, has a generally favorable acute safety profile. Common side effects include nasal irritation, headache, and drowsiness. The acute cardiovascular effects (mild hypotension, slight increase in heart rate) are typically subclinical. Because of its structural similarity to vasopressin, high doses of oxytocin can produce antidiuretic effects, and water retention has been reported with prolonged high-dose administration.
Long-term safety data for chronic intranasal oxytocin use are limited. Theoretical concerns include the possibility of receptor desensitization with repeated use, which could paradoxically impair endogenous oxytocin signaling. Some animal studies have suggested that chronic oxytocin exposure may alter social behavior patterns in ways that persist after discontinuation, raising questions about neuroplastic changes with long-term use.
Current Research Status
Oxytocin is FDA-approved as Pitocin for labor induction and management of postpartum hemorrhage. All other applications, including intranasal use for behavioral and psychiatric indications, remain investigational. Active clinical trials are exploring oxytocin for ASD, social anxiety, PTSD, obesity, chronic pain, and substance use disorders. The peptide is among the most actively researched molecules in neuroscience, though the translation from laboratory findings to approved psychiatric therapies has proven difficult. Intranasal oxytocin formulations are available for research and off-label prescribing through compounding pharmacies.
Frequently Asked Questions
What is oxytocin?
Oxytocin is a natural nine-amino-acid peptide hormone made in the hypothalamus and released from the pituitary, with roles in childbirth, breastfeeding and social behaviour. A synthetic form is an FDA-approved medicine used in hospitals (as Pitocin) mainly to induce or support labour.
How does oxytocin work?
Oxytocin binds the oxytocin receptor, a G-protein coupled receptor that raises intracellular calcium. The receptor is expressed in the uterus, mammary glands and brain, which underlies oxytocin’s roles in contractions, milk release and social signalling.
Is oxytocin FDA-approved?
Oxytocin is FDA-approved as Pitocin for labor induction and management of postpartum hemorrhage. All other applications, including intranasal use for behavioral and psychiatric indications, remain investigational.
What does the research say about oxytocin?
Obstetric use is well established. Behavioral research has reported that intranasal oxytocin can influence trust and social processing, but those findings are investigational and not consistently replicated. Trials are exploring uses such as autism spectrum disorder, social anxiety and PTSD.
What are the safety concerns with oxytocin?
Intravenous oxytocin for labor induction has a well-characterized profile; known risks include uterine hyperstimulation, fetal distress from excessive contractions and, rarely, uterine rupture at high doses. These are dose-dependent effects requiring clinical monitoring.
Research Handling & Storage
Reconstitution (General Guidelines)
Lyophilized peptides are typically reconstituted using bacteriostatic water (0.9% benzyl alcohol). Standard reconstitution protocol:
- Remove the vial from storage and allow it to reach room temperature (20–25°C / 68–77°F) before opening. This typically takes 15–20 minutes.
- Clean the vial stopper with an alcohol prep pad and allow to air dry.
- Using a sterile syringe, slowly inject bacteriostatic water along the inside wall of the vial. Do not spray directly onto the lyophilized powder.
- Gently swirl the vial until the powder is fully dissolved. Do not shake vigorously as this may damage the peptide structure.
- The reconstituted solution should be clear and colorless. Discard if cloudy, discolored, or if particulate matter is visible.
- Label the vial with the reconstitution date, concentration, and your initials.
Common reconstitution volumes in research: 1ml or 2ml of bacteriostatic water per vial, depending on the desired concentration. For example, adding 2ml to a 5mg vial yields a concentration of 2.5mg/ml (2,500mcg/ml).
Storage
- Lyophilized (unreconstituted): Store at -20°C (-4°F) for long-term storage (stable 24+ months), or 2–8°C (36–46°F) refrigerated for short-term storage up to 6 months. Keep desiccated and protected from light.
- Reconstituted: Store at 2–8°C (36–46°F) refrigerated. Use within 4–6 weeks of reconstitution. Do not freeze reconstituted solutions as this may cause degradation.
- Shipping: Lyophilized peptides are generally stable at ambient temperature during transit for several days. Reconstituted solutions should be shipped on ice packs.
Handling Precautions
- Handle with appropriate personal protective equipment (PPE) including nitrile gloves, lab coat, and eye protection.
- Use aseptic/sterile technique when reconstituting and transferring solutions to prevent contamination.
- Avoid repeated freeze-thaw cycles which may denature the compound and reduce potency.
- Keep detailed laboratory records including reconstitution dates, lot numbers, concentrations, and storage conditions.
- Dispose of unused material and sharps in accordance with local regulations and institutional biosafety guidelines.
Stability & Shelf Life
Lyophilized (freeze-dried) peptides are highly stable when stored correctly. At -20°C (-4°F), most peptides retain >95% purity for 24 months or longer. Once reconstituted, the clock starts—proteins in solution are inherently less stable than in dry form. Factors that accelerate degradation include temperature fluctuations, exposure to light, repeated freeze-thaw cycles, bacterial contamination, and oxidation.
Purity & Quality Considerations
Research-grade compounds should be accompanied by a Certificate of Analysis (COA) confirming purity, typically verified by High-Performance Liquid Chromatography (HPLC) and Mass Spectrometry (MS). Look for purity levels of ≥98% for research applications. Third-party testing adds an additional layer of quality assurance. Always verify the source and documentation before using any research compound.
Research Supplies & Resources
Essential supplies and educational resources for peptide research. Links go to Amazon.com.
Lab Supplies
Recommended Reading
Lab Equipment
As an Amazon Associate, peptides.fyi earns from qualifying purchases. Learn more.