Synopsis
Compound overview
- Research only
- In clinical trials
- Approved outside US
- FDA-approved
What it is
Tirzepatide is a dual agonist — a single engineered molecule that activates two gut-hormone receptors at once, GIP and GLP-1. It is FDA-approved and sold by prescription as Mounjaro for diabetes and Zepbound for weight management.
What it does
Its effects are documented in large clinical trials.
- Lowers blood glucose in type 2 diabetes
- Reduces appetite and food intake
- Produced large average weight loss in trials
- Improves metabolic markers such as blood lipids
How it works
By switching on both the GIP and GLP-1 receptors, tirzepatide combines insulin release, slowed digestion and appetite suppression. In head-to-head trials this dual action produced stronger effects than targeting GLP-1 alone.
Safety notes
Tirzepatide is prescription-only. Gastrointestinal side effects — nausea, vomiting, diarrhea — are common, and it carries the same boxed warning for thyroid C-cell tumours as other drugs in its class. It requires medical oversight and gradual dose increases; unregulated research-grade material is not interchangeable with the approved medicine.
Where to buy Tirzepatide
Pre-measured, dial-adjustable dosing — no reconstitution or measuring. The simplest research format to work with.
Standard lyophilized vial — reconstitute and measure doses yourself. The conventional research format.
Affiliate links — we may earn a commission at no extra cost to you.
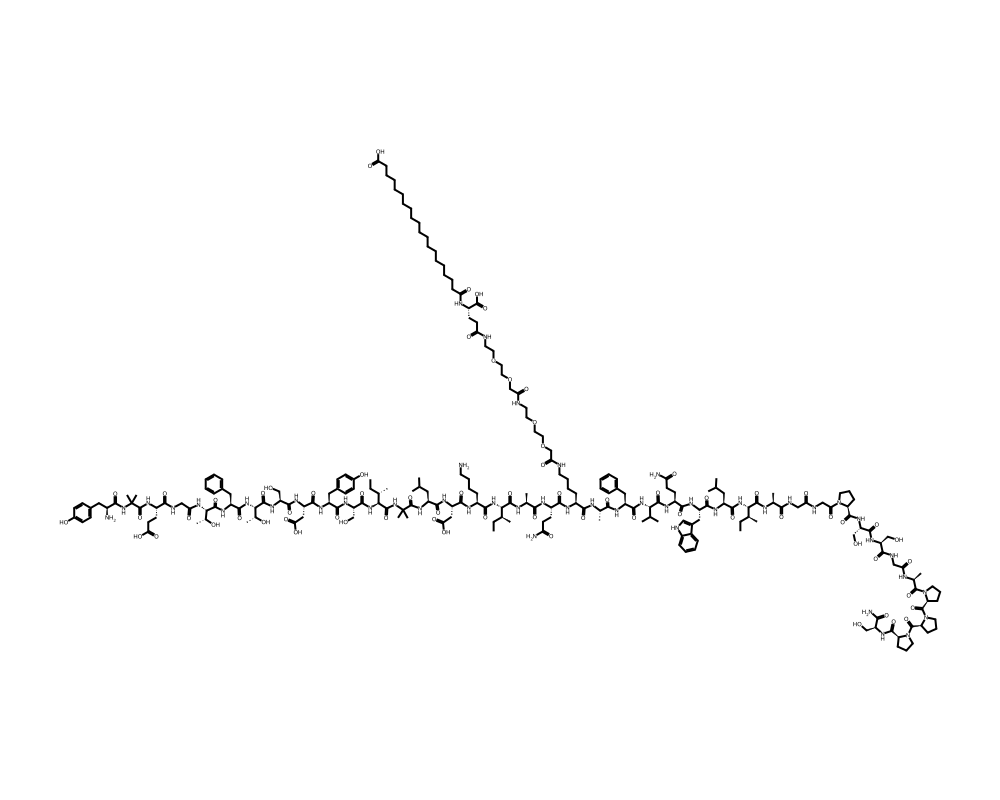
Molecular Structure
Research tool
Reconstitution calculator
Concentration
2.50mg/mL
Draw volume
0.10mL
Insulin units
10IU
Doses/vial
20
Overview
Tirzepatide is a first-in-class dual glucose-dependent insulinotropic polypeptide (GIP) and glucagon-like peptide-1 (GLP-1) receptor agonist developed by Eli Lilly and Company. Often referred to as a “twincretin” due to its engagement of both major incretin receptor systems, tirzepatide represents a paradigm shift in the pharmacological treatment of type 2 diabetes and obesity by harnessing the complementary and synergistic actions of GIP and GLP-1 receptor signaling.
Contents
- Overview
- Mechanism of Action
- GIP Receptor Agonism
- GLP-1 Receptor Agonism
- Synergistic Metabolic Effects
- Research Summary
- SURPASS Program (Type 2 Diabetes)
- SURMOUNT Program (Obesity)
- Obstructive Sleep Apnea
- Heart Failure with Preserved Ejection Fraction
- Dosing in Published Research
- Safety and Side Effects
- Current Research Status
- Frequently Asked Questions
The molecule was approved by the FDA in May 2022 under the brand name Mounjaro for the treatment of type 2 diabetes mellitus, and in November 2023 under the brand name Zepbound for chronic weight management in adults with obesity or overweight with at least one weight-related comorbidity. Its clinical development code was LY3298176.
Tirzepatide is based on the native GIP(1-42) sequence rather than GLP-1, a deliberate design choice by Eli Lilly’s research team led by Dr. Tamer Coskun. The GIP backbone was selected because it provided a more favorable structural scaffold for achieving potent dual agonism. The peptide contains several engineered modifications including non-natural amino acids, a C-20 fatty diacid albumin-binding moiety, and sequence substitutions that confer GLP-1 receptor cross-reactivity while maintaining strong GIP receptor agonism.
Mechanism of Action
Tirzepatide simultaneously activates two incretin receptors with distinct but complementary downstream effects. This dual mechanism produces metabolic benefits that exceed those achievable through GLP-1 receptor agonism alone.
GIP Receptor Agonism
Tirzepatide binds with high affinity to the GIP receptor (GIPR), a class B GPCR expressed on pancreatic beta cells, adipocytes, osteoblasts, and neurons. On beta cells, GIPR activation stimulates cAMP production and potentiates glucose-dependent insulin secretion through PKA and Epac2 pathways, complementing GLP-1R-mediated insulinotropic effects. In adipose tissue, GIP receptor signaling promotes lipid uptake and storage in subcutaneous adipose depots, improving lipid buffering capacity and reducing ectopic fat deposition in liver and visceral compartments. This adipose tissue remodeling effect is thought to improve insulin sensitivity independently of weight loss.
GLP-1 Receptor Agonism
Despite being constructed on a GIP backbone, tirzepatide activates GLP-1R with approximately 5-fold lower potency than native GLP-1, which is nonetheless pharmacologically significant at therapeutic concentrations. GLP-1R activation contributes appetite suppression through hypothalamic and hindbrain circuits, suppresses glucagon secretion, and slows gastric emptying. The combination of GIPR and GLP-1R activation in the central nervous system produces enhanced satiety signaling through convergent neural pathways in the arcuate nucleus and area postrema.
Synergistic Metabolic Effects
Preclinical research by Samms et al. (2021) demonstrated that combined GIP and GLP-1 receptor activation produces synergistic weight loss in diet-induced obese mice that exceeds the additive effects of either receptor system alone. The proposed mechanism involves GIP-mediated enhancement of GLP-1 receptor sensitivity in hypothalamic neurons, amplifying the anorexigenic signal. Additionally, GIP receptor activation in brown and beige adipocytes enhances thermogenic capacity through upregulation of uncoupling protein 1 (UCP-1), contributing to increased energy expenditure.
Research Summary
Tirzepatide has been evaluated in an extensive clinical trial program demonstrating unprecedented efficacy in both glycemic control and weight reduction.
SURPASS Program (Type 2 Diabetes)
The SURPASS Phase III program comprised five pivotal trials evaluating tirzepatide in type 2 diabetes. Frias et al. (2021), published in the New England Journal of Medicine, reported results from SURPASS-2 comparing tirzepatide (5, 10, and 15 mg) to semaglutide 1 mg in 1,879 patients. Tirzepatide at all doses demonstrated superior HbA1c reduction versus semaglutide, with the 15 mg dose achieving a mean HbA1c reduction of 2.46% compared to 1.86% for semaglutide (p<0.001). Weight loss was also significantly greater with tirzepatide 15 mg (-12.4 kg versus -6.2 kg with semaglutide).
SURMOUNT Program (Obesity)
Jastreboff et al. (2022), published in the New England Journal of Medicine, reported SURMOUNT-1 results in 2,539 adults with obesity. At 72 weeks, tirzepatide 15 mg produced a mean weight reduction of 22.5% from baseline compared to 2.4% with placebo. An extraordinary 63% of participants in the 15 mg group achieved at least 20% weight loss, and 36% achieved at least 25% weight loss, outcomes that approach the weight reduction typically achieved with bariatric surgery procedures.
Obstructive Sleep Apnea
Malhotra et al. (2024), published in the New England Journal of Medicine, reported results from the SURMOUNT-OSA trial demonstrating that tirzepatide significantly reduced the apnea-hypopnea index (AHI) in patients with moderate-to-severe obstructive sleep apnea. The 15 mg dose reduced AHI by approximately 50-60% at 52 weeks, with many patients achieving clinically meaningful reductions below the diagnostic threshold, suggesting potential for disease remission in conjunction with weight loss.
Heart Failure with Preserved Ejection Fraction
Kosiborod et al. (2024), published in the New England Journal of Medicine, reported the SUMMIT trial results showing tirzepatide significantly reduced the composite of cardiovascular death or worsening heart failure events by 38% in patients with heart failure with preserved ejection fraction (HFpEF) and obesity, establishing cardiovascular benefit beyond weight management.
Dosing in Published Research
About this section
The information below reports dosing only as it appears in published clinical or preclinical research and official regulatory documents. It is provided as published-literature reference material. It is not dosing guidance, not medical advice, and not a recommendation to use or self-administer this compound.
Tirzepatide is an FDA-approved prescription medicine, sold as Mounjaro for type 2 diabetes and as Zepbound for chronic weight management; both contain the same active drug and use the same titration ladder. The FDA-approved labeling specifies a stepwise schedule:
- 2.5 mg injected subcutaneously once weekly for 4 weeks (a treatment-initiation dose, not a maintenance dose).
- Increase to 5 mg once weekly.
- If further control is needed, increase in 2.5 mg increments after at least 4 weeks at the current dose.
- The labeled maximum is 15 mg once weekly; the full ladder is 2.5, 5, 7.5, 10, 12.5 and 15 mg.
These figures are drawn from FDA-approved prescribing information.
Important
Tirzepatide carries an FDA Boxed Warning for thyroid C-cell tumors and is contraindicated in people with a personal or family history of medullary thyroid carcinoma or with Multiple Endocrine Neoplasia syndrome type 2. The schedule above is part of the approved product and is designed to be followed under the supervision of a prescriber; it is not a recommendation, and it does not apply to material sold for research use.
Safety and Side Effects
Tirzepatide carries an FDA boxed warning, the agency’s most serious warning category, for thyroid C-cell tumors. In rodent studies, tirzepatide caused thyroid C-cell tumors; it is not known whether tirzepatide causes thyroid C-cell tumors, including medullary thyroid carcinoma (MTC), in humans. Tirzepatide is contraindicated in patients with a personal or family history of medullary thyroid carcinoma and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2).
Other labeled risks include
- Acute pancreatitis.
- Gallbladder disease, including gallstones and cholecystitis.
- Acute kidney injury secondary to dehydration.
- Diabetic retinopathy complications in patients with type 2 diabetes.
- Hypoglycemia when combined with insulin or insulin secretagogues.
- Severe gastrointestinal disease.
- Hypersensitivity reactions.
Because tirzepatide delays gastric emptying, it can reduce the effectiveness of oral hormonal contraceptives around the time of initiation and dose escalation. The most common adverse effects are gastrointestinal, including nausea, diarrhea, vomiting, constipation, and abdominal pain, generally dose-related and most pronounced during titration.
As with other agents that produce large reductions in body weight, a portion of the weight lost on tirzepatide is lean (muscle) mass. The drug should be used with caution around pregnancy. Tirzepatide is a prescription medication and should be used only under medical supervision; material sold outside the regulated pharmacy supply chain may differ in identity, dose, and purity from the approved product.
Current Research Status
Tirzepatide is an FDA-approved prescription medication, a dual GIP and GLP-1 receptor agonist approved for type 2 diabetes (Mounjaro) and chronic weight management (Zepbound). It is supported by the SURPASS and SURMOUNT randomized controlled trial programs and by ongoing cardiovascular and heart-failure outcome studies. As with semaglutide, its approval reflects a regulatory benefit-risk judgment for defined populations under medical supervision, and the boxed warning and contraindications above apply.
Further reading: Tirzepatide Microdosing: What the Evidence Shows examines what the research does and does not support regarding lower-dose tirzepatide protocols.
Frequently Asked Questions
What is tirzepatide?
Tirzepatide is a dual agonist, a single engineered molecule that activates two gut-hormone receptors at once, GIP and GLP-1. It is FDA-approved and sold by prescription as Mounjaro for type 2 diabetes and Zepbound for chronic weight management.
How does tirzepatide work?
Tirzepatide simultaneously activates the GIP and GLP-1 receptors, two incretin systems with distinct but complementary effects. Together they improve insulin response, reduce appetite and food intake, and produce metabolic benefits beyond GLP-1 activity alone.
Is tirzepatide FDA-approved?
Yes. Tirzepatide is an FDA-approved prescription medication, approved for type 2 diabetes as Mounjaro and for chronic weight management as Zepbound, with labeling related to cardiovascular risk.
What does the research say about tirzepatide?
Tirzepatide is supported by an extensive trial program: the SURPASS trials in type 2 diabetes and the SURMOUNT trials in weight management, which demonstrated strong effects on glucose control and large average weight loss. Cardiovascular and heart-failure trials are ongoing.
What are the safety concerns with tirzepatide?
Tirzepatide carries an FDA boxed warning for thyroid C-cell tumors, based on rodent studies; whether it causes such tumors in humans is not known. The most common side effects are gastrointestinal, including nausea, vomiting and diarrhea. It is used only under medical supervision.
Research Handling & Storage
Reconstitution (General Guidelines)
Lyophilized peptides are typically reconstituted using bacteriostatic water (0.9% benzyl alcohol). Standard reconstitution protocol:
- Remove the vial from storage and allow it to reach room temperature (20–25°C / 68–77°F) before opening. This typically takes 15–20 minutes.
- Clean the vial stopper with an alcohol prep pad and allow to air dry.
- Using a sterile syringe, slowly inject bacteriostatic water along the inside wall of the vial. Do not spray directly onto the lyophilized powder.
- Gently swirl the vial until the powder is fully dissolved. Do not shake vigorously as this may damage the peptide structure.
- The reconstituted solution should be clear and colorless. Discard if cloudy, discolored, or if particulate matter is visible.
- Label the vial with the reconstitution date, concentration, and your initials.
Common reconstitution volumes in research: 1ml or 2ml of bacteriostatic water per vial, depending on the desired concentration. For example, adding 2ml to a 5mg vial yields a concentration of 2.5mg/ml (2,500mcg/ml).
Storage
- Lyophilized (unreconstituted): Store at -20°C (-4°F) for long-term storage (stable 24+ months), or 2–8°C (36–46°F) refrigerated for short-term storage up to 6 months. Keep desiccated and protected from light.
- Reconstituted: Store at 2–8°C (36–46°F) refrigerated. Use within 4–6 weeks of reconstitution. Do not freeze reconstituted solutions as this may cause degradation.
- Shipping: Lyophilized peptides are generally stable at ambient temperature during transit for several days. Reconstituted solutions should be shipped on ice packs.
Handling Precautions
- Handle with appropriate personal protective equipment (PPE) including nitrile gloves, lab coat, and eye protection.
- Use aseptic/sterile technique when reconstituting and transferring solutions to prevent contamination.
- Avoid repeated freeze-thaw cycles which may denature the compound and reduce potency.
- Keep detailed laboratory records including reconstitution dates, lot numbers, concentrations, and storage conditions.
- Dispose of unused material and sharps in accordance with local regulations and institutional biosafety guidelines.
Stability & Shelf Life
Lyophilized (freeze-dried) peptides are highly stable when stored correctly. At -20°C (-4°F), most peptides retain >95% purity for 24 months or longer. Once reconstituted, the clock starts—proteins in solution are inherently less stable than in dry form. Factors that accelerate degradation include temperature fluctuations, exposure to light, repeated freeze-thaw cycles, bacterial contamination, and oxidation.
Purity & Quality Considerations
Research-grade compounds should be accompanied by a Certificate of Analysis (COA) confirming purity, typically verified by High-Performance Liquid Chromatography (HPLC) and Mass Spectrometry (MS). Look for purity levels of ≥98% for research applications. Third-party testing adds an additional layer of quality assurance. Always verify the source and documentation before using any research compound.
Research Supplies & Resources
Essential supplies and educational resources for peptide research. Links go to Amazon.com.
Lab Supplies
Recommended Reading
Lab Equipment
As an Amazon Associate, peptides.fyi earns from qualifying purchases. Learn more.