Synopsis
Compound overview
- Research only
- In clinical trials
- Approved outside US
- FDA-approved
What it is
Semaglutide is a GLP-1 receptor agonist — a lab-made molecule that closely mimics GLP-1, a hormone the gut releases after eating. Unlike most compounds on this site, it is a fully FDA-approved medicine, sold by prescription as Ozempic, Wegovy and Rybelsus.
What it does
Its effects are well documented across large clinical trials.
- Lowers blood sugar in type 2 diabetes
- Reduces appetite and overall food intake
- Supports significant weight loss
- Slows how quickly the stomach empties
How it works
Semaglutide switches on the GLP-1 receptor. That prompts the pancreas to release insulin when blood sugar is high, slows stomach emptying so meals feel longer-lasting, and signals fullness to the brain — together reducing both blood sugar and appetite.
Safety notes
Semaglutide is prescription-only for good reason. Nausea, vomiting and diarrhea are common, especially early on, and it carries a boxed warning over a risk of thyroid C-cell tumours seen in rodents. It is meant to be used under medical supervision with dose titration and monitoring; research-vendor material is not pharmacy-grade and is no substitute for a prescription.
Where to buy Semaglutide
Standard lyophilized vial — reconstitute and measure doses yourself. The conventional research format.
Affiliate links — we may earn a commission at no extra cost to you.
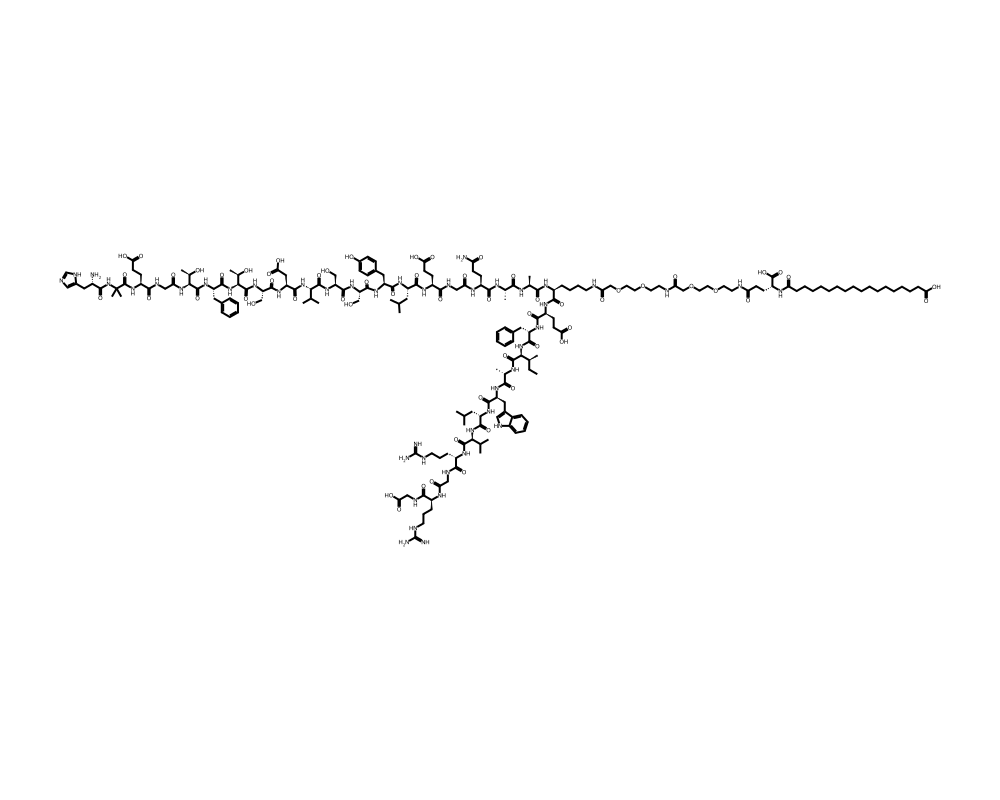
Molecular Structure
Research tool
Reconstitution calculator
Concentration
2.50mg/mL
Draw volume
0.10mL
Insulin units
10IU
Doses/vial
20
Overview
Semaglutide is a long-acting glucagon-like peptide-1 (GLP-1) receptor agonist developed by Novo Nordisk. It is a synthetic analogue of human GLP-1(7-37) with three key structural modifications that dramatically extend its pharmacokinetic half-life from approximately 2 minutes (native GLP-1) to roughly 7 days, enabling once-weekly subcutaneous administration or once-daily oral dosing.
Contents
- Overview
- Mechanism of Action
- Pancreatic Effects
- Central Appetite Regulation
- Gastric Motility
- Research Summary
- SUSTAIN Program (Type 2 Diabetes)
- STEP Program (Weight Management)
- SELECT Cardiovascular Trial
- Oral Semaglutide (PIONEER Program)
- Dosing in Published Research
- Safety and Side Effects
- Current Research Status
- Frequently Asked Questions
The molecule was first approved by the FDA in December 2017 under the brand name Ozempic for the treatment of type 2 diabetes mellitus. In June 2021, a higher-dose formulation received FDA approval under the brand name Wegovy specifically for chronic weight management in adults with obesity (BMI greater than or equal to 30 kg/m2) or overweight (BMI greater than or equal to 27 kg/m2) with at least one weight-related comorbidity. An oral formulation, Rybelsus, was approved in September 2019, making it the first GLP-1 receptor agonist available in tablet form.
Semaglutide represents the culmination of decades of incretin biology research that began with the discovery of the incretin effect by Elrick et al. in 1964 and the isolation of GLP-1 by Mojsov, Habener, and colleagues in 1986-1987. Its development built upon the prior success of liraglutide (Victoza/Saxenda), incorporating additional modifications that conferred superior pharmacokinetic and clinical properties.
Mechanism of Action
Semaglutide activates the GLP-1 receptor (GLP-1R), a class B G protein-coupled receptor expressed in pancreatic beta cells, the gastrointestinal tract, the heart, kidneys, and critically, in multiple brain regions involved in appetite regulation and reward processing.
Pancreatic Effects
Upon binding to GLP-1R on pancreatic beta cells, semaglutide stimulates glucose-dependent insulin secretion through the cAMP/PKA and Epac2 signaling pathways. This glucose-dependent mechanism means insulin release is potentiated only when blood glucose is elevated, significantly reducing the risk of hypoglycemia compared to sulfonylureas or exogenous insulin. Simultaneously, semaglutide suppresses glucagon secretion from alpha cells during hyperglycemia through both direct GLP-1R activation on alpha cells and paracrine effects mediated by somatostatin release from delta cells.
Central Appetite Regulation
Semaglutide crosses the blood-brain barrier and activates GLP-1R in hypothalamic nuclei (arcuate nucleus, paraventricular nucleus) and hindbrain areas (nucleus tractus solitarius, area postrema). In the arcuate nucleus, it activates anorexigenic POMC/CART neurons while inhibiting orexigenic NPY/AgRP neurons. Critically, emerging research by Drucker and colleagues has shown that semaglutide also modulates mesolimbic dopaminergic reward circuitry, reducing food-related reward signaling in the ventral tegmental area and nucleus accumbens, which may explain observed reductions in cravings and hedonic eating behaviors.
Gastric Motility
GLP-1R activation in the enteric nervous system and vagal afferent pathways slows gastric emptying, prolonging gastric distension and activating mechanosensitive satiety signals. This deceleration of gastric emptying also contributes to reduced postprandial glucose excursions by slowing the rate of nutrient delivery to the absorptive surfaces of the small intestine.
Research Summary
Semaglutide has one of the most extensive clinical evidence bases of any peptide therapeutic, with multiple large-scale randomized controlled trials completed across diabetes, obesity, cardiovascular, and renal disease indications.
SUSTAIN Program (Type 2 Diabetes)
The SUSTAIN clinical trial program comprised multiple Phase III studies evaluating semaglutide in type 2 diabetes. SUSTAIN-6, published by Marso et al. (2016) in the New England Journal of Medicine, was a cardiovascular outcomes trial enrolling 3,297 patients that demonstrated a statistically significant 26% reduction in major adverse cardiovascular events (MACE) with semaglutide versus placebo (HR 0.74, 95% CI 0.58-0.95, p=0.02). Mean HbA1c reductions ranged from 1.0-1.8% across the SUSTAIN trials.
STEP Program (Weight Management)
The STEP (Semaglutide Treatment Effect in People with Obesity) program established semaglutide 2.4 mg weekly as a transformative weight management therapy. Wilding et al. (2021), published in the New England Journal of Medicine, reported results from STEP 1: among 1,961 adults with obesity, semaglutide produced a mean weight loss of 14.9% from baseline at 68 weeks compared to 2.4% with placebo (p<0.001). Approximately one-third of participants achieved weight loss of 20% or greater, approaching outcomes previously achievable only with bariatric surgery.
SELECT Cardiovascular Trial
Lincoff et al. (2023), published in the New England Journal of Medicine, reported results from the SELECT trial, a landmark study of 17,604 adults with established cardiovascular disease and overweight/obesity but without diabetes. Semaglutide 2.4 mg weekly reduced the risk of MACE by 20% (HR 0.80, 95% CI 0.72-0.90, p<0.001), establishing for the first time that a weight management intervention could reduce cardiovascular events independently of diabetes treatment.
Oral Semaglutide (PIONEER Program)
The PIONEER trial program evaluated oral semaglutide co-formulated with sodium N-(8-[2-hydroxybenzoyl]amino) caprylate (SNAC), an absorption enhancer that facilitates gastric absorption of the peptide. Husain et al. (2019) published the PIONEER 6 cardiovascular safety trial in the New England Journal of Medicine, demonstrating non-inferiority to placebo for cardiovascular safety with a point estimate suggesting potential benefit (HR 0.79, 95% CI 0.57-1.11).
Dosing in Published Research
About this section
The information below reports dosing only as it appears in published clinical or preclinical research and official regulatory documents. It is provided as published-literature reference material. It is not dosing guidance, not medical advice, and not a recommendation to use or self-administer this compound.
Semaglutide is an FDA-approved prescription medicine, sold as Ozempic and Rybelsus for type 2 diabetes and as Wegovy for chronic weight management. Its dosing is set by approved product labeling. For Wegovy (a subcutaneous injection), the FDA-approved labeling specifies a gradual escalation intended to improve gastrointestinal tolerability:
- 0.25 mg once weekly for 4 weeks (a treatment-initiation dose, not a maintenance dose).
- 0.5 mg once weekly for 4 weeks.
- 1 mg once weekly for 4 weeks.
- 1.7 mg once weekly for 4 weeks.
- 2.4 mg once weekly as the maintenance dose.
For Ozempic (type 2 diabetes), labeling starts at 0.25 mg once weekly for 4 weeks, then 0.5 mg, then 1 mg, with a 2 mg option for additional glycemic control. These figures are drawn from FDA-approved prescribing information.
Important
Semaglutide carries an FDA Boxed Warning for thyroid C-cell tumors and is contraindicated in people with a personal or family history of medullary thyroid carcinoma or with Multiple Endocrine Neoplasia syndrome type 2. The escalation schedule above is part of the approved product and is designed to be followed under the supervision of a prescriber; it is not a recommendation, and it does not apply to material sold for research use.
Safety and Side Effects
Semaglutide carries an FDA boxed warning, the agency’s most serious warning category, for thyroid C-cell tumors. In rodent studies, semaglutide caused dose-dependent and treatment-duration-dependent thyroid C-cell tumors, including medullary thyroid carcinoma. It is not known whether semaglutide causes thyroid C-cell tumors, including medullary thyroid carcinoma (MTC), in humans, because the human relevance of the rodent finding could not be determined. Semaglutide is contraindicated in patients with a personal or family history of medullary thyroid carcinoma and in patients with Multiple Endocrine Neoplasia syndrome type 2 (MEN 2).
Other labeled risks include
- Acute pancreatitis.
- Gallbladder disease, including gallstones and cholecystitis, associated both with the drug and with rapid weight loss.
- Acute kidney injury, often in the setting of dehydration from vomiting or diarrhea.
- Diabetic retinopathy complications in patients with type 2 diabetes.
- Ileus.
- Hypoglycemia when used together with insulin or sulfonylureas.
- Hypersensitivity reactions.
The most common adverse effects are gastrointestinal, including nausea, vomiting, diarrhea, constipation, and abdominal pain, which are generally dose-related and most pronounced during dose escalation.
As with other interventions that produce substantial weight loss, a meaningful proportion of the weight lost is lean (muscle) mass, an effect that remains an active area of research. Semaglutide should generally be discontinued before a planned pregnancy because of its long half-life and limited human pregnancy data. It is a prescription medication and should be used only under medical supervision; products sold outside the regulated pharmacy supply chain, including compounded or research-labeled material, may differ in identity, dose, and purity from the approved product.
Current Research Status
Semaglutide is an FDA-approved prescription medication. It is approved for type 2 diabetes (Ozempic injectable and Rybelsus oral) and for chronic weight management (Wegovy), with additional labeling related to cardiovascular risk reduction. It is supported by a large body of randomized controlled trial evidence, including dedicated cardiovascular outcome trials. Its approval reflects a regulatory judgment that benefits outweigh risks for defined patient populations under medical supervision; the boxed warning and labeled contraindications described above apply.
Further reading: GLP-1 Drugs and Muscle Loss: The Research on Lean Mass reviews what trials report about lean mass changes during GLP-1 receptor agonist treatment.
Frequently Asked Questions
What is semaglutide?
Semaglutide is a GLP-1 receptor agonist, a lab-made molecule that closely mimics GLP-1, a hormone the gut releases after eating. It is a fully FDA-approved medicine, sold by prescription as Ozempic, Wegovy and Rybelsus.
How does semaglutide work?
Semaglutide activates the GLP-1 receptor, which is found in the pancreas, gut and brain regions involved in appetite. This improves insulin response in type 2 diabetes, reduces appetite and food intake, and slows stomach emptying.
Is semaglutide FDA-approved?
Yes. Semaglutide is FDA-approved for type 2 diabetes (Ozempic injectable and Rybelsus oral) and for chronic weight management (Wegovy), with additional labeling related to cardiovascular risk reduction.
What does the research say about semaglutide?
Semaglutide has one of the most extensive evidence bases of any peptide therapeutic, including the SUSTAIN trials in type 2 diabetes and large trials in obesity, cardiovascular and renal disease, which documented improvements in blood sugar, weight and related outcomes.
What are the safety concerns with semaglutide?
Semaglutide carries an FDA boxed warning for thyroid C-cell tumors, based on rodent studies; whether it causes such tumors in humans is not known. The most common side effects are gastrointestinal, including nausea. It is a prescription medicine used under medical supervision.
Research Handling & Storage
Reconstitution (General Guidelines)
Lyophilized peptides are typically reconstituted using bacteriostatic water (0.9% benzyl alcohol). Standard reconstitution protocol:
- Remove the vial from storage and allow it to reach room temperature (20–25°C / 68–77°F) before opening. This typically takes 15–20 minutes.
- Clean the vial stopper with an alcohol prep pad and allow to air dry.
- Using a sterile syringe, slowly inject bacteriostatic water along the inside wall of the vial. Do not spray directly onto the lyophilized powder.
- Gently swirl the vial until the powder is fully dissolved. Do not shake vigorously as this may damage the peptide structure.
- The reconstituted solution should be clear and colorless. Discard if cloudy, discolored, or if particulate matter is visible.
- Label the vial with the reconstitution date, concentration, and your initials.
Common reconstitution volumes in research: 1ml or 2ml of bacteriostatic water per vial, depending on the desired concentration. For example, adding 2ml to a 5mg vial yields a concentration of 2.5mg/ml (2,500mcg/ml).
Storage
- Lyophilized (unreconstituted): Store at -20°C (-4°F) for long-term storage (stable 24+ months), or 2–8°C (36–46°F) refrigerated for short-term storage up to 6 months. Keep desiccated and protected from light.
- Reconstituted: Store at 2–8°C (36–46°F) refrigerated. Use within 4–6 weeks of reconstitution. Do not freeze reconstituted solutions as this may cause degradation.
- Shipping: Lyophilized peptides are generally stable at ambient temperature during transit for several days. Reconstituted solutions should be shipped on ice packs.
Handling Precautions
- Handle with appropriate personal protective equipment (PPE) including nitrile gloves, lab coat, and eye protection.
- Use aseptic/sterile technique when reconstituting and transferring solutions to prevent contamination.
- Avoid repeated freeze-thaw cycles which may denature the compound and reduce potency.
- Keep detailed laboratory records including reconstitution dates, lot numbers, concentrations, and storage conditions.
- Dispose of unused material and sharps in accordance with local regulations and institutional biosafety guidelines.
Stability & Shelf Life
Lyophilized (freeze-dried) peptides are highly stable when stored correctly. At -20°C (-4°F), most peptides retain >95% purity for 24 months or longer. Once reconstituted, the clock starts—proteins in solution are inherently less stable than in dry form. Factors that accelerate degradation include temperature fluctuations, exposure to light, repeated freeze-thaw cycles, bacterial contamination, and oxidation.
Purity & Quality Considerations
Research-grade compounds should be accompanied by a Certificate of Analysis (COA) confirming purity, typically verified by High-Performance Liquid Chromatography (HPLC) and Mass Spectrometry (MS). Look for purity levels of ≥98% for research applications. Third-party testing adds an additional layer of quality assurance. Always verify the source and documentation before using any research compound.
Research Supplies & Resources
Essential supplies and educational resources for peptide research. Links go to Amazon.com.
Lab Supplies
Recommended Reading
Lab Equipment
As an Amazon Associate, peptides.fyi earns from qualifying purchases. Learn more.