Synopsis
Compound overview
- Research only
- In clinical trials
- Approved outside US
- FDA-approved
What it is
TB-500 is a synthetic peptide based on an active fragment of thymosin beta-4, a protein the body produces that plays a role in cell repair. The research chemical sold as "TB-500" is this lab-made fragment, not the complete natural protein. It is not approved as a drug.
What it does
Claims for TB-500 rest almost entirely on animal and lab research.
- Tissue and wound repair in rodents
- Movement of repair cells toward injury sites
- Reported recovery and flexibility effects
- Formation of new blood vessels
How it works
Thymosin beta-4 binds actin, a protein central to cell movement and structure. This is thought to help cells migrate to damaged tissue and rebuild it. How faithfully the shorter TB-500 fragment reproduces that effect in humans is not established.
Safety notes
No completed human trials exist for TB-500, so its safety profile in people is unknown. It is on the WADA prohibited list for athletes, and research-grade purity varies between suppliers. Human use should be considered experimental.
Where to buy TB-500
Standard lyophilized vial — reconstitute and measure doses yourself. The conventional research format.
Affiliate links — we may earn a commission at no extra cost to you.
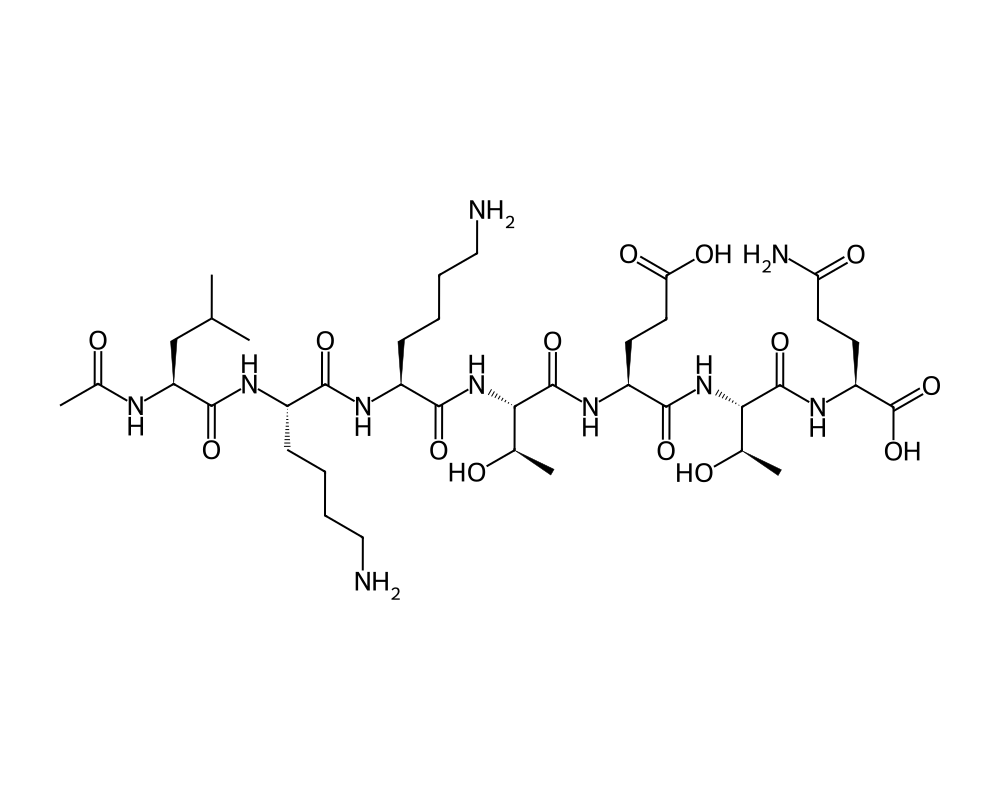
Molecular Structure
Research tool
Reconstitution calculator
Concentration
2.50mg/mL
Draw volume
0.10mL
Insulin units
10IU
Doses/vial
20
Overview
TB-500 is a synthetic version of Thymosin Beta-4 (Tb4), a naturally occurring 43-amino acid peptide that is one of the most abundant intracellular proteins in mammalian cells. Thymosin Beta-4 was originally isolated from the thymus gland by Allan Goldstein and colleagues at the George Washington University in the 1960s, though it was later discovered to be expressed ubiquitously throughout the body and not limited to thymic tissue.
Contents
- Overview
- Mechanism of Action
- Actin Sequestration and Dynamics
- Cell Migration and Angiogenesis
- Anti-inflammatory Properties
- Research Summary
- Wound Healing
- Cardiac Repair
- Corneal Healing
- Neurological Recovery
- Dosing in Published Research
- Safety and Side Effects
- Current Research Status
- Frequently Asked Questions
Tb4 is the primary G-actin sequestering peptide in eukaryotic cells, maintaining a reservoir of monomeric actin (G-actin) that can be rapidly mobilized for cytoskeletal reorganization. This fundamental role in actin dynamics gives Tb4 influence over virtually every process that depends on cellular motility and structural remodeling, including wound healing, angiogenesis, inflammation, and cardiac repair.
The synthetic form, TB-500, replicates the full 43-amino acid sequence of endogenous Tb4. It has been the subject of extensive research in wound healing, corneal repair, cardiac regeneration, and neurological recovery. RegeneRx Biopharmaceuticals advanced Tb4-based therapeutics through multiple clinical trials, including Phase II studies for dry eye syndrome and cardiac repair following myocardial infarction.
Mechanism of Action
TB-500 exerts its biological effects through multiple interconnected mechanisms centered on actin cytoskeleton regulation and downstream signaling pathways.
Actin Sequestration and Dynamics
The primary biochemical function of Tb4 is sequestering monomeric G-actin in a 1:1 complex, preventing its spontaneous polymerization into F-actin filaments. The central actin-binding domain of Tb4, the sequence LKKTETQ (residues 17-23), is critical for this interaction. By maintaining the G-actin pool, Tb4 enables rapid cytoskeletal remodeling when cells need to migrate, divide, or change shape in response to tissue injury.
Cell Migration and Angiogenesis
Tb4 promotes both endothelial and epithelial cell migration, which are essential for wound closure and new blood vessel formation. The pro-migratory effect involves activation of integrin-linked kinase (ILK) and Akt/protein kinase B signaling. Phosphorylated Akt promotes cell survival, migration, and the expression of matrix metalloproteinases (MMPs) that facilitate tissue remodeling. Tb4 also stimulates VEGF expression, promoting angiogenesis at wound sites.
Anti-inflammatory Properties
Tb4 modulates inflammatory responses by downregulating pro-inflammatory chemokines and cytokines at wound sites. It reduces neutrophil infiltration and decreases the expression of inflammatory mediators including IL-1b, TNF-a, and MIP-2. This anti-inflammatory activity helps shift the wound environment from a destructive inflammatory phase to a constructive reparative phase.
Research Summary
Wound Healing
Malinda et al. (1999), publishing in the Journal of Investigative Dermatology, conducted the landmark study demonstrating Tb4’s wound healing properties. Topical application of Tb4 to full-thickness dermal wounds in rats accelerated wound closure by 4-6 days compared to controls. Histological analysis revealed enhanced angiogenesis, collagen deposition, and keratinocyte migration in treated wounds. This study opened a new field of Tb4 wound healing research.
Cardiac Repair
Bock-Marquette et al. (2004), in a landmark paper published in Nature, demonstrated that Tb4 promoted survival of cardiomyocytes following myocardial infarction in mice. Intraperitoneal injection of Tb4 after coronary artery ligation reduced infarct size and improved cardiac function. The mechanism involved Akt activation and subsequent inhibition of apoptotic pathways. This study initiated clinical development for cardiac applications.
Corneal Healing
Sosne et al. (2002), in Investigative Ophthalmology & Visual Science, showed that Tb4 promoted corneal epithelial wound healing and reduced inflammation in rat models of corneal injury. Phase II clinical trials conducted by RegeneRx for dry eye syndrome (RGN-259 eye drops) showed that topical Tb4 significantly improved corneal staining scores and symptom questionnaire results compared to placebo, as reported by Dunn et al. (2010) in Ophthalmology.
Neurological Recovery
Xiong et al. (2012), publishing in the Journal of Neuroscience Research, demonstrated that Tb4 treatment improved functional neurological recovery following traumatic brain injury in rats. The treated animals showed enhanced neurogenesis, oligodendrogenesis, and angiogenesis in the injured brain regions. Tb4 also promoted axonal remodeling and synaptic plasticity, contributing to improved motor and cognitive outcomes measured over 35 days post-injury.
Dosing in Published Research
About this section
The information below reports dosing only as it appears in published clinical or preclinical research and official regulatory documents. It is provided as published-literature reference material. It is not dosing guidance, not medical advice, and not a recommendation to use or self-administer this compound.
TB-500 is a synthetic peptide based on a fragment of the natural protein thymosin beta-4. Although recombinant thymosin beta-4 itself has been examined in early-phase human studies, no controlled human trial has established a dose for the TB-500 fragment for the muscle, tendon or ligament uses commonly discussed. Because human dosing for TB-500 has not been defined in the published literature, specific figures circulating in vendor material are unverified and are not reported here.
No established human dosing
Because no controlled human trial has established a dose for TB-500, any specific figures circulating online are unverified. TB-500 is not an approved drug product, is prohibited in sport by WADA, and injectable material sold under this name is for laboratory research use only.
Safety and Side Effects
Human safety data for TB-500 are essentially absent; the evidence base is preclinical, primarily in animal models, and controlled clinical trials have not characterized its adverse-effect profile. A specific theoretical concern follows from its proposed mechanism: TB-500 and the related thymosin beta-4 fragment promote angiogenesis and cell migration. These processes are central to wound healing, but they are also processes that tumors exploit, so a systemically administered agent with these properties carries a theoretical risk of promoting the growth or spread of an existing malignancy, a concern that has not been resolved in humans. Injectable research-chemical material is also subject to sterility, identity, and purity problems.
Current Research Status
TB-500 is not approved by the FDA or any major regulatory agency for any use. Thymosin beta-4 itself has been studied in clinical trials for indications such as dry eye and wound healing, but TB-500 as sold is not that approved-pathway product. TB-500 is prohibited in sport by the World Anti-Doping Agency. It should be regarded as an investigational compound with unestablished human efficacy and safety.
Further reading: TB-500 appears alongside GHK-Cu, BPC-157, and KPV in the KLOW peptide blend.
Frequently Asked Questions
What is TB-500?
TB-500 is a synthetic peptide based on an active fragment of thymosin beta-4, a naturally occurring protein involved in cell repair. The research chemical sold as TB-500 is this lab-made fragment, not the complete natural protein, and it is not approved as a drug.
How does TB-500 work?
TB-500 is linked to regulation of actin, a structural protein central to cell movement. Through actin dynamics and related signalling it is proposed to support the migration of repair cells and the formation of new blood vessels, based mainly on animal and laboratory research.
Is TB-500 FDA-approved?
No. TB-500 is not approved by the FDA or any major regulatory agency for any use, and it is prohibited in sport by WADA. Thymosin beta-4 itself has been studied in clinical trials, but TB-500 as sold is not that approved-pathway product.
What does the research say about TB-500?
Claims for TB-500 rest almost entirely on animal and laboratory research. A landmark study (Malinda et al., 1999) reported that topical thymosin beta-4 accelerated wound closure in rats. Controlled human trials of TB-500 have not been conducted.
What are the safety concerns with TB-500?
Human safety data are essentially absent; the evidence base is preclinical, and controlled clinical trials have not characterized its adverse-effect profile. A theoretical concern relates to its proposed mechanism and effects on cell migration, which has not been resolved.
Research Handling & Storage
Reconstitution (General Guidelines)
Lyophilized peptides are typically reconstituted using bacteriostatic water (0.9% benzyl alcohol). Standard reconstitution protocol:
- Remove the vial from storage and allow it to reach room temperature (20–25°C / 68–77°F) before opening. This typically takes 15–20 minutes.
- Clean the vial stopper with an alcohol prep pad and allow to air dry.
- Using a sterile syringe, slowly inject bacteriostatic water along the inside wall of the vial. Do not spray directly onto the lyophilized powder.
- Gently swirl the vial until the powder is fully dissolved. Do not shake vigorously as this may damage the peptide structure.
- The reconstituted solution should be clear and colorless. Discard if cloudy, discolored, or if particulate matter is visible.
- Label the vial with the reconstitution date, concentration, and your initials.
Common reconstitution volumes in research: 1ml or 2ml of bacteriostatic water per vial, depending on the desired concentration. For example, adding 2ml to a 5mg vial yields a concentration of 2.5mg/ml (2,500mcg/ml).
Storage
- Lyophilized (unreconstituted): Store at -20°C (-4°F) for long-term storage (stable 24+ months), or 2–8°C (36–46°F) refrigerated for short-term storage up to 6 months. Keep desiccated and protected from light.
- Reconstituted: Store at 2–8°C (36–46°F) refrigerated. Use within 4–6 weeks of reconstitution. Do not freeze reconstituted solutions as this may cause degradation.
- Shipping: Lyophilized peptides are generally stable at ambient temperature during transit for several days. Reconstituted solutions should be shipped on ice packs.
Handling Precautions
- Handle with appropriate personal protective equipment (PPE) including nitrile gloves, lab coat, and eye protection.
- Use aseptic/sterile technique when reconstituting and transferring solutions to prevent contamination.
- Avoid repeated freeze-thaw cycles which may denature the compound and reduce potency.
- Keep detailed laboratory records including reconstitution dates, lot numbers, concentrations, and storage conditions.
- Dispose of unused material and sharps in accordance with local regulations and institutional biosafety guidelines.
Stability & Shelf Life
Lyophilized (freeze-dried) peptides are highly stable when stored correctly. At -20°C (-4°F), most peptides retain >95% purity for 24 months or longer. Once reconstituted, the clock starts—proteins in solution are inherently less stable than in dry form. Factors that accelerate degradation include temperature fluctuations, exposure to light, repeated freeze-thaw cycles, bacterial contamination, and oxidation.
Purity & Quality Considerations
Research-grade compounds should be accompanied by a Certificate of Analysis (COA) confirming purity, typically verified by High-Performance Liquid Chromatography (HPLC) and Mass Spectrometry (MS). Look for purity levels of ≥98% for research applications. Third-party testing adds an additional layer of quality assurance. Always verify the source and documentation before using any research compound.
Research Supplies & Resources
Essential supplies and educational resources for peptide research. Links go to Amazon.com.
Lab Supplies
Recommended Reading
Lab Equipment
As an Amazon Associate, peptides.fyi earns from qualifying purchases. Learn more.