Synopsis
Compound overview
- Research only
- In clinical trials
- Approved outside US
- FDA-approved
What it is
GHRP-2 (pralmorelin) is a synthetic growth-hormone-releasing peptide. It is not approved as a treatment in the US; in Japan a single-dose version is approved only as a diagnostic test for growth-hormone deficiency. Elsewhere it is sold as a research chemical.
What it does
Effects observed in research include:
- Prompts the pituitary to release growth hormone
- Strongly stimulates appetite
- Studied as a growth-hormone-deficiency diagnostic
- Often combined with GHRH peptides in research
How it works
GHRP-2 activates the ghrelin (growth-hormone-secretagogue) receptor in the pituitary gland, triggering a pulse of growth-hormone release while also signalling hunger to the brain.
Safety notes
Outside its narrow diagnostic use, GHRP-2 has no approved-medicine safety record. Reported effects include increased hunger, water retention and a rise in the hormones cortisol and prolactin. It is banned in sport, and research-grade purity varies between suppliers.
Where to buy GHRP-2
Standard lyophilized vial — reconstitute and measure doses yourself. The conventional research format.
Affiliate links — we may earn a commission at no extra cost to you.
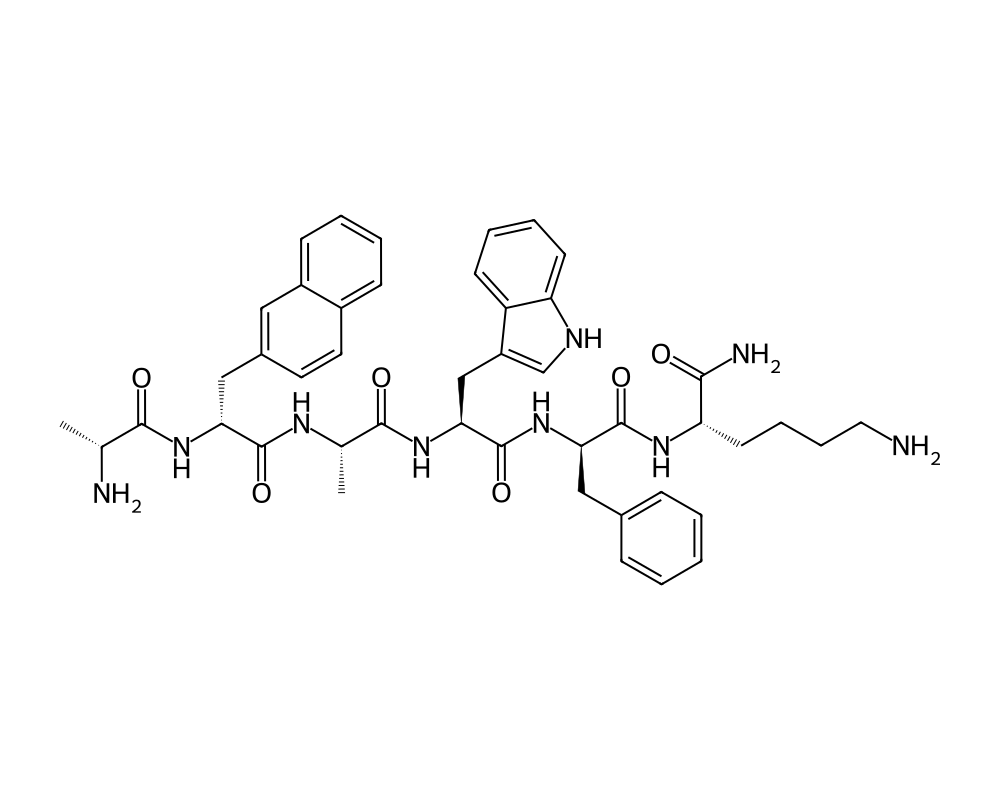
Molecular Structure
Research tool
Reconstitution calculator
Concentration
2.50mg/mL
Draw volume
0.10mL
Insulin units
10IU
Doses/vial
20
Overview
GHRP-2 (Growth Hormone Releasing Peptide-2), also known by its pharmaceutical name Pralmorelin, is a synthetic hexapeptide that functions as a potent growth hormone secretagogue and ghrelin receptor agonist. It was developed as a second-generation improvement upon GHRP-6, offering enhanced GH-releasing potency with a somewhat improved side-effect profile.
Contents
- Overview
- Mechanism of Action
- Ghrelin Receptor Agonism
- Somatostatin Antagonism
- GHRH Synergy
- Research Summary
- Diagnostic Utility
- Comparative GH Secretagogue Studies
- Cortisol and Prolactin Effects
- Age-Related GH Decline
- Dosing in Published Research
- Safety and Side Effects
- Current Research Status
- Frequently Asked Questions
GHRP-2 holds a unique distinction among the growth hormone releasing peptides: it is the only GHRP to have received regulatory approval for clinical use, having been approved in Japan under the trade name GHRP Kaken 100 as a diagnostic agent for growth hormone deficiency. The Japanese approval, granted by the Pharmaceuticals and Medical Devices Agency (PMDA), validated the compound’s pharmacological activity and safety profile in clinical settings.
Among the GHRP family, GHRP-2 is considered the most potent GH releaser on a per-milligram basis. It stimulates GH secretion more robustly than GHRP-6 and with less appetite stimulation, though it shares the tendency to modestly elevate cortisol and prolactin at supraphysiological doses. GHRP-2 has been widely used as a research tool in endocrinology for over three decades to study the GH secretagogue receptor system and to probe GH axis function.
Mechanism of Action
GHRP-2 stimulates growth hormone release through a multi-level mechanism involving both the pituitary gland and the hypothalamus.
Ghrelin Receptor Agonism
GHRP-2 is a potent agonist of the growth hormone secretagogue receptor type 1a (GHS-R1a), the endogenous ligand of which is ghrelin. Binding to GHS-R1a activates the Gq/11-phospholipase C signaling cascade, generating inositol trisphosphate (IP3) and diacylglycerol (DAG). IP3 mobilizes calcium from intracellular stores, while DAG activates protein kinase C. The resulting elevation in intracellular calcium triggers fusion of GH-containing secretory vesicles with the plasma membrane.
Somatostatin Antagonism
A distinctive feature of GHRP-2 is its functional antagonism of somatostatin signaling. While GHRP-2 does not directly bind somatostatin receptors, it reduces somatostatin tone through hypothalamic mechanisms. This effectively lifts the inhibitory brake on GH secretion, which explains why GHRPs can stimulate GH release even during periods of high somatostatin activity when GHRH alone is ineffective.
GHRH Synergy
GHRP-2 and GHRH act through complementary intracellular pathways in somatotrophs. GHRH activates adenylyl cyclase and the cAMP-PKA pathway, while GHRP-2 activates the PLC-IP3-calcium pathway. When administered together, these agents produce synergistic GH release that exceeds the sum of their individual effects. This pharmacological synergy has been extensively documented in both animal and human studies.
Research Summary
Diagnostic Utility
Doi et al. (2004), publishing in the Journal of Clinical Endocrinology & Metabolism, evaluated GHRP-2 as a diagnostic tool for GH deficiency in Japanese adults. Intravenous administration of 100 mcg GHRP-2 reliably distinguished GH-deficient patients from healthy controls, with a sensitivity of 93% and specificity of 89% using a GH cutoff of 15 ng/mL. This study supported the regulatory approval of GHRP-2 as a diagnostic agent in Japan.
Comparative GH Secretagogue Studies
Bowers et al. (1994), in a seminal paper in the Journal of Clinical Endocrinology & Metabolism, compared the GH-releasing activity of GHRP-2, GHRP-6, and GHRH in healthy adults. GHRP-2 produced the highest peak GH levels (approximately 70-80 ng/mL at 1 mcg/kg IV) compared to GHRP-6 (approximately 40-60 ng/mL) and GHRH alone (approximately 20-30 ng/mL). The combination of GHRP-2 plus GHRH produced GH peaks exceeding 100 ng/mL in these studies.
Cortisol and Prolactin Effects
Arvat et al. (1997), publishing in the European Journal of Endocrinology, characterized the neuroendocrine profile of GHRP-2 in humans. At GH-stimulating doses (1 mcg/kg), GHRP-2 produced modest elevations in cortisol (approximately 30-50% above baseline) and prolactin (approximately 40-80% above baseline), both of which were transient and normalized within 2-3 hours. These effects were less pronounced than those of GHRP-6 at equipotent GH-releasing doses.
Age-Related GH Decline
Broglio et al. (2003), in European Journal of Endocrinology, investigated GHRP-2 in elderly subjects and found that while the absolute GH response was reduced compared to young adults (consistent with age-related somatopause), GHRP-2 still produced clinically meaningful GH elevations. The relative response to GHRP-2 was better preserved with aging than the response to GHRH alone, suggesting that the ghrelin pathway remains more functionally intact in older individuals.
Dosing in Published Research
About this section
The information below reports dosing only as it appears in published clinical or preclinical research and official regulatory documents. It is provided as published-literature reference material. It is not dosing guidance, not medical advice, and not a recommendation to use or self-administer this compound.
GHRP-2, also known as pralmorelin, is a synthetic growth-hormone-releasing peptide. It is not approved in the United States. It is, however, approved in Japan as a diagnostic agent for assessing growth-hormone secretory capacity, where the labeled use is a single 100 microgram intravenous bolus, given as part of a GH-stimulation test in adults and children. That regimen was established in Japanese multicenter trials. These figures describe approved diagnostic use in Japan and the trials supporting it.
Research doses, not a protocol
The 100 microgram figure is a single-use diagnostic dose given under medical supervision, not an established regimen for repeated or therapeutic use. GHRP-2 is not FDA-approved, and material sold for research use is not a regulated drug product.
Safety and Side Effects
GHRP-2 has not been established as safe through completed clinical development. As a growth hormone secretagogue and ghrelin-receptor agonist it shares the class effects of fluid retention, altered insulin sensitivity and blood glucose, headache, and injection-site reactions, and it stimulates appetite, though generally less intensely than GHRP-6. It produces modest increases in cortisol and prolactin. Sustained elevation of growth hormone and IGF-1 carries the theoretical metabolic and proliferative concerns common to the class. Long-term human safety data do not exist, and research-chemical material is of uncertain identity and purity.
Current Research Status
GHRP-2 reached early clinical investigation, including use as a diagnostic agent for growth hormone secretion in some countries, but it is not approved by the FDA or as a therapeutic in major markets. It is prohibited in sport by the World Anti-Doping Agency. It is sold as a research chemical and should be regarded as investigational for any other purpose.
Frequently Asked Questions
What is GHRP-2?
GHRP-2, also called pralmorelin, is a synthetic growth-hormone-releasing peptide. It is not approved as a treatment in the United States; in Japan a single-dose version is approved only as a diagnostic test for growth-hormone deficiency. Elsewhere it is sold as a research chemical.
How does GHRP-2 work?
GHRP-2 activates the growth hormone secretagogue receptor (GHS-R1a), the same receptor as the natural hormone ghrelin, acting on both the pituitary and hypothalamus to prompt growth hormone release. It also strongly stimulates appetite.
Is GHRP-2 FDA-approved?
No. GHRP-2 reached early clinical investigation and is used as a diagnostic agent for growth hormone secretion in some countries, but it is not approved by the FDA or as a therapeutic in major markets. It is prohibited in sport by WADA.
What does the research say about GHRP-2?
A study by Doi and colleagues (2004) found that intravenous GHRP-2 reliably distinguished growth-hormone-deficient patients from healthy controls, supporting its diagnostic use. It is often combined with GHRH peptides in research, but it has no completed therapeutic development program.
What are the safety concerns with GHRP-2?
GHRP-2 has not been established as safe through completed clinical development. As a growth hormone secretagogue it shares class effects including fluid retention, altered insulin sensitivity and blood glucose, headache, injection-site reactions and increased appetite.
Research Handling & Storage
Reconstitution (General Guidelines)
Lyophilized peptides are typically reconstituted using bacteriostatic water (0.9% benzyl alcohol). Standard reconstitution protocol:
- Remove the vial from storage and allow it to reach room temperature (20–25°C / 68–77°F) before opening. This typically takes 15–20 minutes.
- Clean the vial stopper with an alcohol prep pad and allow to air dry.
- Using a sterile syringe, slowly inject bacteriostatic water along the inside wall of the vial. Do not spray directly onto the lyophilized powder.
- Gently swirl the vial until the powder is fully dissolved. Do not shake vigorously as this may damage the peptide structure.
- The reconstituted solution should be clear and colorless. Discard if cloudy, discolored, or if particulate matter is visible.
- Label the vial with the reconstitution date, concentration, and your initials.
Common reconstitution volumes in research: 1ml or 2ml of bacteriostatic water per vial, depending on the desired concentration. For example, adding 2ml to a 5mg vial yields a concentration of 2.5mg/ml (2,500mcg/ml).
Storage
- Lyophilized (unreconstituted): Store at -20°C (-4°F) for long-term storage (stable 24+ months), or 2–8°C (36–46°F) refrigerated for short-term storage up to 6 months. Keep desiccated and protected from light.
- Reconstituted: Store at 2–8°C (36–46°F) refrigerated. Use within 4–6 weeks of reconstitution. Do not freeze reconstituted solutions as this may cause degradation.
- Shipping: Lyophilized peptides are generally stable at ambient temperature during transit for several days. Reconstituted solutions should be shipped on ice packs.
Handling Precautions
- Handle with appropriate personal protective equipment (PPE) including nitrile gloves, lab coat, and eye protection.
- Use aseptic/sterile technique when reconstituting and transferring solutions to prevent contamination.
- Avoid repeated freeze-thaw cycles which may denature the compound and reduce potency.
- Keep detailed laboratory records including reconstitution dates, lot numbers, concentrations, and storage conditions.
- Dispose of unused material and sharps in accordance with local regulations and institutional biosafety guidelines.
Stability & Shelf Life
Lyophilized (freeze-dried) peptides are highly stable when stored correctly. At -20°C (-4°F), most peptides retain >95% purity for 24 months or longer. Once reconstituted, the clock starts—proteins in solution are inherently less stable than in dry form. Factors that accelerate degradation include temperature fluctuations, exposure to light, repeated freeze-thaw cycles, bacterial contamination, and oxidation.
Purity & Quality Considerations
Research-grade compounds should be accompanied by a Certificate of Analysis (COA) confirming purity, typically verified by High-Performance Liquid Chromatography (HPLC) and Mass Spectrometry (MS). Look for purity levels of ≥98% for research applications. Third-party testing adds an additional layer of quality assurance. Always verify the source and documentation before using any research compound.
Research Supplies & Resources
Essential supplies and educational resources for peptide research. Links go to Amazon.com.
Lab Supplies
Recommended Reading
Lab Equipment
As an Amazon Associate, peptides.fyi earns from qualifying purchases. Learn more.