Synopsis
Compound overview
- Research only
- In clinical trials
- Approved outside US
- FDA-approved
What it is
Tesamorelin is a synthetic, stabilised analogue of growth-hormone-releasing hormone (GHRH). It is FDA-approved and sold by prescription as Egrifta, used to reduce excess abdominal fat in people with HIV-associated lipodystrophy.
What it does
Documented effects from clinical use include:
- Reduces visceral (deep abdominal) fat in its approved use
- Prompts the body's own growth-hormone release
- Studied for effects on liver fat
- Has documented clinical-trial data
How it works
Tesamorelin binds the GHRH receptor on the pituitary gland, prompting a natural, pulsed release of growth hormone, which in turn influences how the body stores and burns fat.
Safety notes
Tesamorelin is prescription-only. Reported side effects include joint pain, swelling, injection-site reactions and changes in blood sugar. It is approved for a specific medical condition under medical supervision; research-vendor material is not pharmacy-grade.
Where to buy Tesamorelin
Standard lyophilized vial — reconstitute and measure doses yourself. The conventional research format.
Affiliate links — we may earn a commission at no extra cost to you.
Molecular Structure
Overview
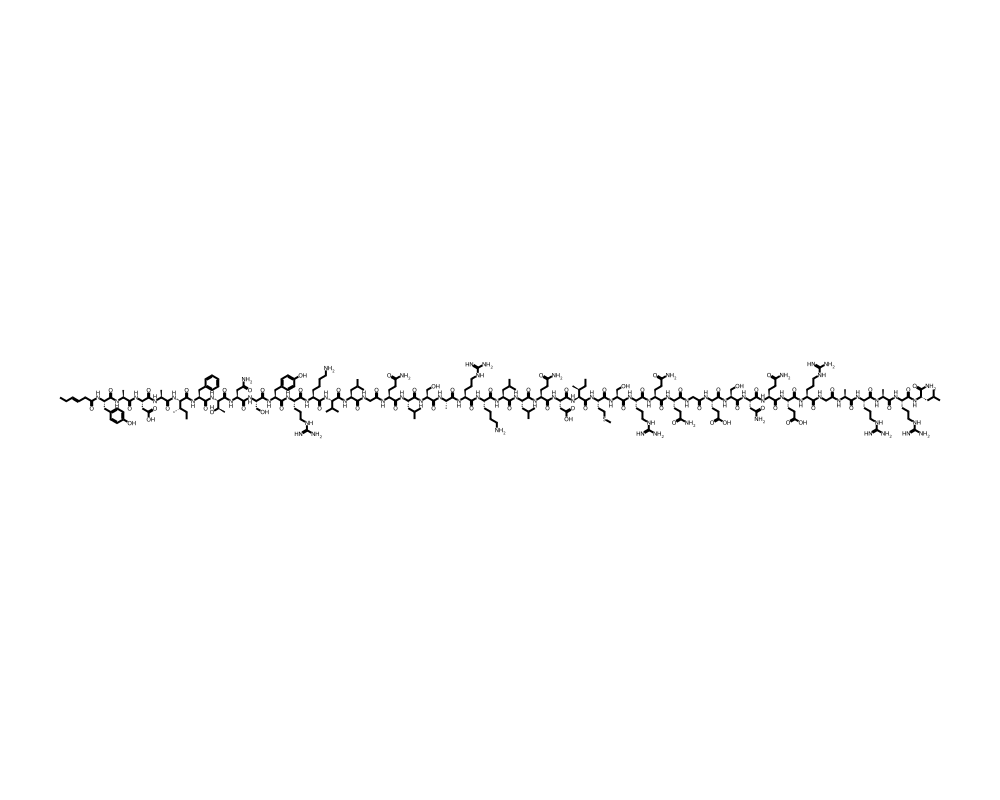
Tesamorelin is a synthetic analog of human growth hormone-releasing hormone (GHRH), consisting of the full 44-amino acid sequence of endogenous GHRH(1-44) with a trans-3-hexenoic acid modification at the N-terminus. This structural modification enhances the peptide’s resistance to enzymatic degradation by dipeptidyl peptidase-IV (DPP-IV), substantially increasing its biological half-life compared to native GHRH.
Contents
- Overview
- Mechanism of Action
- Pituitary Stimulation and GH Release
- Lipolytic Pathway Activation
- Metabolic Effects
- Research Summary
- HIV-Associated Lipodystrophy
- Hepatic Steatosis and NAFLD
- Cognitive Function
- Body Composition and Cardiometabolic Risk
- Dosing in Published Research
- Safety and Side Effects
- Current Research Status
- Frequently Asked Questions
Developed by Theratechnologies Inc. of Montreal, Canada, Tesamorelin was approved by the U.S. Food and Drug Administration in November 2010 under the brand name Egrifta for the reduction of excess abdominal fat in HIV-infected patients with lipodystrophy. It remains the only GHRH analog with full FDA approval for a clinical indication, distinguishing it from other growth hormone secretagogues that remain in preclinical or investigational stages.
The peptide functions by stimulating the anterior pituitary gland to synthesize and release endogenous growth hormone (GH) in a pulsatile, physiological manner. This mechanism preserves the hypothalamic-pituitary feedback axis, a significant advantage over exogenous GH administration, which can suppress endogenous production and disrupt normal regulatory pathways. Tesamorelin’s ability to restore near-physiological GH secretion patterns has made it an important subject in endocrinology and metabolic disease research.
Mechanism of Action
Tesamorelin’s pharmacological activity centers on its high-affinity binding to the GHRH receptor (GHRH-R), a G protein-coupled receptor expressed predominantly on somatotroph cells of the anterior pituitary gland.
Pituitary Stimulation and GH Release
Upon binding to the GHRH receptor, Tesamorelin activates the adenylyl cyclase-cAMP-protein kinase A signaling cascade. This leads to calcium influx through voltage-gated calcium channels, triggering exocytosis of growth hormone-containing secretory granules. The resulting GH release follows a pulsatile pattern that mirrors natural secretion dynamics, which is critical for maintaining downstream signaling fidelity at peripheral tissues. Studies by Koutkia et al. (2004), published in the Journal of Clinical Endocrinology and Metabolism, confirmed that Tesamorelin produces dose-dependent increases in circulating GH and IGF-1 levels.
Lipolytic Pathway Activation
The GH released in response to Tesamorelin stimulation activates lipolytic pathways in visceral adipose tissue. Growth hormone binds to GH receptors on adipocytes, activating hormone-sensitive lipase (HSL) through JAK2-STAT5 signaling. This promotes the hydrolysis of stored triglycerides into free fatty acids and glycerol, preferentially targeting visceral fat depots. Research has demonstrated that visceral adipocytes express higher densities of GH receptors compared to subcutaneous fat, explaining the selective reduction of trunk fat observed in clinical trials.
Metabolic Effects
Beyond direct lipolysis, Tesamorelin-induced GH secretion modulates hepatic lipid metabolism, reducing intrahepatic fat content and improving markers of liver function. IGF-1 elevation secondary to GH stimulation also contributes to improved insulin sensitivity in peripheral tissues, though GH itself can transiently increase insulin resistance, creating a complex metabolic balance that has been the subject of extensive clinical investigation.
Research Summary
HIV-Associated Lipodystrophy
The pivotal Phase III clinical trials that led to FDA approval were published by Falutz et al. (2007) in the Journal of the American Medical Association (JAMA). In a multicenter, randomized, double-blind, placebo-controlled study involving 412 HIV-infected patients with excess abdominal fat, Tesamorelin 2 mg administered subcutaneously once daily for 26 weeks produced a statistically significant reduction in visceral adipose tissue (VAT) of approximately 15.2% compared to a 5.0% increase in the placebo group (p < 0.001). Patients also reported improvements in body image perception and trunk fat ratios. Importantly, the treatment did not adversely affect glucose metabolism or HIV viral load.
Hepatic Steatosis and NAFLD
Stanley et al. (2014), publishing in The Lancet HIV, conducted a randomized controlled trial examining Tesamorelin’s effects on liver fat content in HIV-positive patients. Over 12 months, Tesamorelin reduced hepatic fat fraction by 37% as measured by magnetic resonance spectroscopy, compared to a 10% increase in the placebo group. The study also demonstrated improvements in liver fibrosis biomarkers and reductions in circulating inflammatory markers including C-reactive protein and interleukin-6, suggesting potential hepatoprotective effects beyond simple fat reduction.
Cognitive Function
An emerging area of Tesamorelin research involves its effects on cognitive function. Cognition and the GH/IGF-1 axis are closely linked, and GH deficiency has been associated with impaired memory and executive function. Dhillon (2011), in a comprehensive review published in Drugs, noted that Tesamorelin’s ability to restore physiological GH/IGF-1 levels could have neuroprotective implications. Subsequent pilot studies in adults with mild cognitive impairment have shown promising trends in verbal memory and executive function tasks, though larger controlled trials are needed to establish definitive cognitive benefits.
Body Composition and Cardiometabolic Risk
Longer-term extension studies have demonstrated that continued Tesamorelin treatment maintains reductions in visceral fat for up to 12 months, with partial reversal upon discontinuation. Falutz et al. (2008) reported that the VAT reduction was accompanied by favorable changes in triglyceride levels, with a mean decrease of 50 mg/dL, and improvements in the ratio of total cholesterol to HDL cholesterol. These findings suggest that Tesamorelin may confer cardiovascular risk reduction beyond its direct effects on adiposity.
Dosing in Published Research
About this section
The information below reports dosing only as it appears in published clinical or preclinical research and official regulatory documents. It is provided as published-literature reference material. It is not dosing guidance, not medical advice, and not a recommendation to use or self-administer this compound.
Tesamorelin is an FDA-approved prescription medicine, sold as Egrifta. According to the FDA-approved labeling, the dose is 2 mg injected subcutaneously into the abdomen once daily, for the reduction of excess abdominal fat in people with HIV-associated lipodystrophy. In the pivotal trials, this regimen reduced visceral adipose tissue by roughly 15 to 18 percent over 26 weeks. These figures are drawn from FDA-approved prescribing information.
Important
The 2 mg daily dose applies to the approved prescription product, studied in a specific HIV-associated lipodystrophy population under medical supervision. It is not a recommendation, and it does not apply to material sold for laboratory or research use, which is not the approved drug product.
Safety and Side Effects
Tesamorelin is an FDA-approved drug with a characterized safety profile. As a growth-hormone-releasing hormone analog it raises growth hormone and IGF-1, and its labeled risks reflect this: elevated IGF-1, the potential for glucose intolerance and worsening of diabetes, fluid retention and edema, joint pain (arthralgia), and musculoskeletal discomfort. Injection-site reactions and hypersensitivity reactions are reported. Because it stimulates the growth hormone and IGF-1 axis, tesamorelin is contraindicated in people with active malignancy, in those with certain disruptions of the hypothalamic-pituitary axis, and in pregnancy; IGF-1 levels are monitored during treatment. It is not indicated for general weight loss.
Current Research Status
Tesamorelin is an FDA-approved prescription medication, marketed as Egrifta, approved for the reduction of excess abdominal fat in people with HIV-associated lipodystrophy. Its approval is specific to that indication; use for general fat loss, bodybuilding, or anti-aging is off-label and not supported by the approval. As a prescription drug it should be used under medical supervision.
Frequently Asked Questions
What is tesamorelin?
Tesamorelin is a synthetic, stabilized analog of growth-hormone-releasing hormone (GHRH). It is FDA-approved and sold by prescription as Egrifta, used to reduce excess abdominal fat in people with HIV-associated lipodystrophy.
How does tesamorelin work?
Tesamorelin binds the GHRH receptor on the pituitary gland, prompting the body to release its own growth hormone. A structural modification makes it resistant to rapid breakdown, extending its activity compared with natural GHRH.
Is tesamorelin FDA-approved?
Yes, for one specific use. Tesamorelin is FDA-approved as Egrifta for the reduction of excess abdominal fat in people with HIV-associated lipodystrophy. Use for general fat loss, bodybuilding or anti-aging is off-label and not supported by its approval.
What does the research say about tesamorelin?
The pivotal Phase III trials (Falutz et al., 2007, JAMA), a randomized, double-blind, placebo-controlled study in 412 HIV-infected patients with abdominal fat accumulation, supported its approved use. It has also been studied for effects on liver fat.
What are the safety concerns with tesamorelin?
Because it raises growth hormone and IGF-1, its labeled risks reflect this, including elevated IGF-1, the potential for glucose intolerance or worsening of diabetes, fluid retention and edema, and joint pain. It is a prescription drug used under medical supervision.
Research Handling & Storage
Storage
- Unopened: Store at controlled room temperature, 20–25°C (68–77°F), away from direct sunlight, heat, and moisture.
- Opened: Keep container tightly closed. Use within the timeframe indicated on the label, typically 30–90 days after opening.
- Do not freeze liquid solutions unless specifically indicated.
Handling Precautions
- Handle with appropriate personal protective equipment (PPE) including nitrile gloves, lab coat, and eye protection.
- Use aseptic/sterile technique when reconstituting and transferring solutions to prevent contamination.
- Avoid repeated freeze-thaw cycles which may denature the compound and reduce potency.
- Keep detailed laboratory records including reconstitution dates, lot numbers, concentrations, and storage conditions.
- Dispose of unused material and sharps in accordance with local regulations and institutional biosafety guidelines.
Stability & Shelf Life
Liquid formulations typically remain stable for 1–2 years when stored at the recommended temperature in the original sealed container. Once opened, potency may gradually decrease. Monitor for any changes in color, clarity, or odor, which may indicate degradation.
Purity & Quality Considerations
Research-grade compounds should be accompanied by a Certificate of Analysis (COA) confirming purity, typically verified by High-Performance Liquid Chromatography (HPLC) and Mass Spectrometry (MS). Look for purity levels of ≥98% for research applications. Third-party testing adds an additional layer of quality assurance. Always verify the source and documentation before using any research compound.
Research Supplies & Resources
Essential supplies and educational resources for peptide research. Links go to Amazon.com.
Lab Supplies
Recommended Reading
Lab Equipment
As an Amazon Associate, peptides.fyi earns from qualifying purchases. Learn more.