Synopsis
Compound overview
- Research only
- In clinical trials
- Approved outside US
- FDA-approved
What it is
Hexarelin is a synthetic growth-hormone-releasing peptide, closely related to the GHRP family. It was investigated in clinical research but never approved as a drug, and is sold only as a research chemical.
What it does
Areas explored in research include:
- Triggers growth-hormone release
- Studied for effects on heart tissue in early research
- Shorter human track record than GHRP-2 or GHRP-6
- Often grouped with other secretagogues
How it works
Hexarelin activates the ghrelin receptor in the pituitary to stimulate growth-hormone release. Research has also examined receptors in heart tissue, though that work is preliminary.
Safety notes
Hexarelin has no approved-medicine safety record. Studies suggest its growth-hormone effect can fade with continued use, and it may raise cortisol and prolactin. It is banned in sport, and research-grade purity varies.
Where to buy Hexarelin
Standard lyophilized vial — reconstitute and measure doses yourself. The conventional research format.
Affiliate links — we may earn a commission at no extra cost to you.
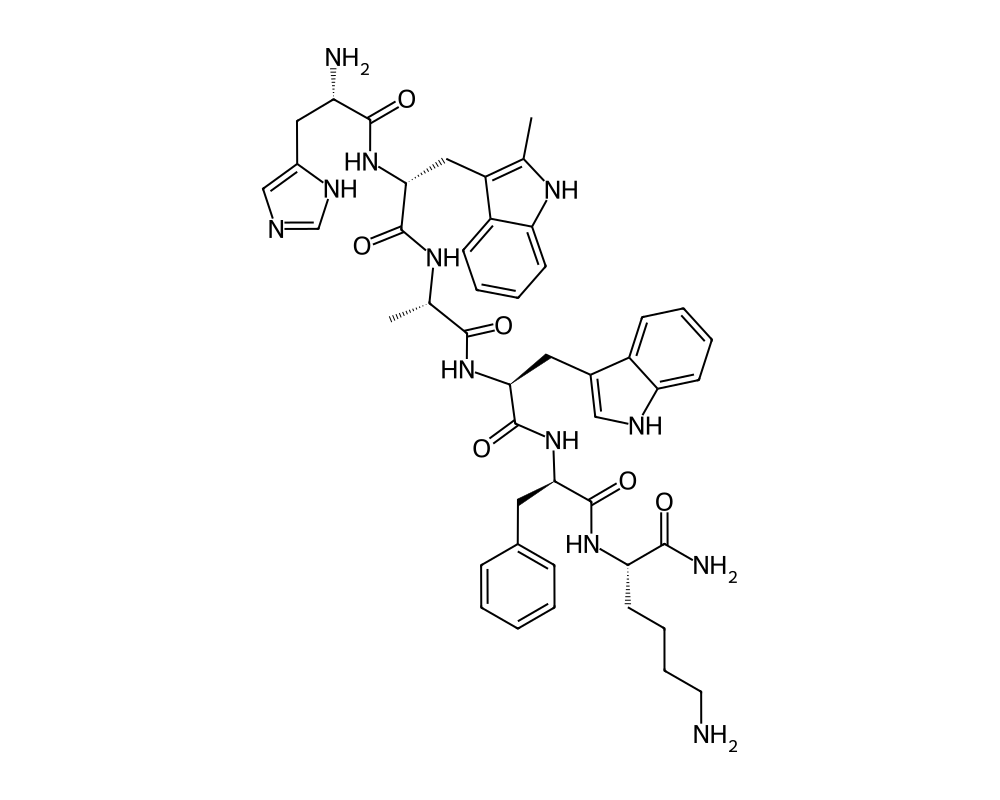
Molecular Structure
Research tool
Reconstitution calculator
Concentration
2.50mg/mL
Draw volume
0.10mL
Insulin units
10IU
Doses/vial
20
Overview
Hexarelin is a synthetic hexapeptide growth hormone secretagogue that has attracted considerable attention from endocrinologists and pharmaceutical researchers since its development in the 1990s. Structurally derived from GHRP-6, hexarelin was engineered to resist enzymatic degradation more effectively than its predecessor, giving it a longer functional half-life and stronger growth hormone (GH) releasing potency. It belongs to a class of compounds known as growth hormone secretagogue receptor (GHSR) agonists, meaning it binds to the same receptor targeted by ghrelin, the so-called “hunger hormone” produced in the stomach.
Contents
What distinguishes hexarelin from other GH-releasing peptides is its potency. Studies have consistently shown that hexarelin is among the most powerful synthetic GH secretagogues available, producing reliable and significant elevations in plasma GH concentrations even at relatively modest doses. It was originally developed by Mediolanum Farmaceutici in Italy and has been the subject of numerous clinical investigations spanning cardiac health, endocrine function, and metabolic regulation.
Hexarelin does not require co-administration with a growth hormone-releasing hormone (GHRH) analog to exert its effects, though combining the two produces synergistic GH release. This independence from GHRH pathways is one of the reasons researchers have found hexarelin to be a particularly useful tool for probing the mechanisms of GH secretion in both healthy subjects and patients with pituitary disorders.
Mechanism of Action
Hexarelin exerts its primary effects by binding to the growth hormone secretagogue receptor type 1a (GHS-R1a), a G-protein coupled receptor found in the hypothalamus and pituitary gland. Activation of this receptor triggers a signaling cascade that involves phospholipase C, inositol triphosphate, and intracellular calcium mobilization, ultimately leading to the release of growth hormone from somatotroph cells in the anterior pituitary.
The mechanism differs meaningfully from that of GHRH, which acts through a separate receptor (the GHRH receptor) and relies on cyclic AMP as its primary second messenger. Because hexarelin and GHRH work through distinct intracellular pathways, their effects on GH release are additive or even synergistic when administered together. This has made the combination a valuable research tool for studying the full secretory capacity of the pituitary.
Beyond the pituitary, hexarelin has demonstrated direct effects on cardiac tissue. Research has identified GHS-R1a expression in cardiomyocytes, and hexarelin binding appears to activate protective signaling pathways in the heart, including those involving Akt and ERK1/2. These cardioprotective effects appear to operate independently of growth hormone release, suggesting hexarelin has biological activities that extend well beyond its role as a GH secretagogue.
Hexarelin also influences cortisol and prolactin levels, though these effects tend to diminish with repeated dosing. ACTH and cortisol elevations are observed acutely but attenuate with chronic administration, while the GH response, though it also diminishes somewhat over time, remains clinically significant.
Research Summary
Clinical research on hexarelin spans several domains. In healthy young adults, single subcutaneous injections of hexarelin at doses between 1 and 2 micrograms per kilogram reliably produced GH peaks of 40 to 80 ng/mL, substantially higher than those achieved with GHRP-6 at equivalent doses. Studies in elderly subjects showed attenuated but still meaningful GH responses, consistent with the known age-related decline in GH secretory capacity.
Cardiac research has been among the most intriguing areas of hexarelin investigation. A series of studies conducted at Italian research institutions demonstrated that hexarelin administration improved cardiac output and reduced systemic vascular resistance in patients with heart failure. In animal models of ischemia-reperfusion injury, hexarelin pretreatment significantly reduced infarct size and preserved left ventricular function. These findings suggested that hexarelin might have therapeutic potential in cardiovascular disease independent of its GH-releasing properties.
Research in GH-deficient populations has shown that hexarelin can be used as a diagnostic tool to assess residual pituitary function. Because its mechanism bypasses the GHRH receptor, hexarelin stimulation testing can help differentiate between hypothalamic and pituitary causes of GH deficiency.
Metabolic studies have explored hexarelin’s effects on body composition and lipid profiles. Animal research has shown reductions in visceral fat and improvements in insulin sensitivity following chronic hexarelin administration, though these findings have not been extensively replicated in controlled human trials.
Dosing in Published Research
About this section
The information below reports dosing only as it appears in published clinical or preclinical research and official regulatory documents. It is provided as published-literature reference material. It is not dosing guidance, not medical advice, and not a recommendation to use or self-administer this compound.
Hexarelin is a synthetic growth-hormone-releasing peptide. It is not an approved medicine and has no labeled dose. It has, however, been examined in published human pharmacology studies. In a controlled dose-response study, single intravenous boluses of 0.5, 1 and 2 micrograms per kilogram of body weight were given to adult volunteers; growth-hormone release rose with dose, and the 2 micrograms-per-kilogram dose produced a near-maximal response. These figures describe what was administered in that specific study.
Research doses, not a protocol
These are doses used in short controlled pharmacology studies, not an established or recommended regimen. Hexarelin has not been developed into an approved drug, and material sold for research use is not a regulated drug product.
Safety and Side Effects
In clinical trials, hexarelin has generally been well tolerated. The most commonly reported side effects include transient facial flushing, mild increases in appetite, and occasional dizziness at the time of injection. These effects are typically self-limiting and resolve within minutes to hours.
The acute elevations in cortisol and prolactin observed with initial hexarelin dosing have raised theoretical concerns about chronic use, but studies of repeated administration over periods of weeks have shown that these hormonal perturbations diminish substantially with continued use. The attenuation of the GH response itself with chronic dosing (a phenomenon common to all GH secretagogues) is considered a practical limitation rather than a safety concern per se.
No significant adverse cardiac events have been reported in clinical studies, and the cardioprotective data, while preliminary, are encouraging from a safety standpoint. Water retention and joint discomfort, side effects associated with elevated GH levels generally, have been reported anecdotally but were not prominent findings in controlled research settings.
Long-term safety data remain limited. The majority of human studies have involved relatively short treatment periods of days to weeks, and comprehensive data on the effects of months or years of hexarelin use do not exist in the published literature.
Current Research Status
Hexarelin remains a research compound without regulatory approval for clinical use in any major market. It has not advanced through the full phases of clinical development required for pharmaceutical approval, despite a relatively robust body of early-phase clinical data. Current research interest centers on its cardioprotective properties and its utility as a diagnostic agent in endocrinology. The peptide continues to be commercially available through research chemical suppliers and is used in laboratory settings for studies of GH physiology and cardiac biology. No active Phase III clinical trials are currently registered for hexarelin.
Frequently Asked Questions
What is hexarelin?
Hexarelin, also called examorelin, is a synthetic hexapeptide growth hormone secretagogue, closely related to the GHRP family and structurally derived from GHRP-6. It was investigated in clinical research but was never approved as a drug, and is sold only as a research chemical.
How does hexarelin work?
Hexarelin binds the growth hormone secretagogue receptor (GHS-R1a) in the hypothalamus and pituitary, triggering a signalling cascade that prompts the pituitary to release growth hormone. It activates the same receptor as the natural hormone ghrelin.
Is hexarelin FDA-approved?
No. Hexarelin remains a research compound without regulatory approval for clinical use in any major market. Despite a relatively robust body of early-phase clinical data, it never advanced through the full phases of pharmaceutical development.
What does the research say about hexarelin?
In healthy young adults, single subcutaneous injections produced large growth-hormone peaks, higher than GHRP-6 at equivalent doses. It has also been studied for effects on heart tissue in early research, but it has a shorter human track record than GHRP-2 or GHRP-6.
What are the safety concerns with hexarelin?
In clinical trials hexarelin was generally well tolerated, with the most common side effects being transient facial flushing, mild increases in appetite and occasional dizziness around the time of injection. Long-term safety has not been established because development never progressed to later-phase trials.
Research Handling & Storage
Reconstitution (General Guidelines)
Lyophilized peptides are typically reconstituted using bacteriostatic water (0.9% benzyl alcohol). Standard reconstitution protocol:
- Remove the vial from storage and allow it to reach room temperature (20–25°C / 68–77°F) before opening. This typically takes 15–20 minutes.
- Clean the vial stopper with an alcohol prep pad and allow to air dry.
- Using a sterile syringe, slowly inject bacteriostatic water along the inside wall of the vial. Do not spray directly onto the lyophilized powder.
- Gently swirl the vial until the powder is fully dissolved. Do not shake vigorously as this may damage the peptide structure.
- The reconstituted solution should be clear and colorless. Discard if cloudy, discolored, or if particulate matter is visible.
- Label the vial with the reconstitution date, concentration, and your initials.
Common reconstitution volumes in research: 1ml or 2ml of bacteriostatic water per vial, depending on the desired concentration. For example, adding 2ml to a 5mg vial yields a concentration of 2.5mg/ml (2,500mcg/ml).
Storage
- Lyophilized (unreconstituted): Store at -20°C (-4°F) for long-term storage (stable 24+ months), or 2–8°C (36–46°F) refrigerated for short-term storage up to 6 months. Keep desiccated and protected from light.
- Reconstituted: Store at 2–8°C (36–46°F) refrigerated. Use within 4–6 weeks of reconstitution. Do not freeze reconstituted solutions as this may cause degradation.
- Shipping: Lyophilized peptides are generally stable at ambient temperature during transit for several days. Reconstituted solutions should be shipped on ice packs.
Handling Precautions
- Handle with appropriate personal protective equipment (PPE) including nitrile gloves, lab coat, and eye protection.
- Use aseptic/sterile technique when reconstituting and transferring solutions to prevent contamination.
- Avoid repeated freeze-thaw cycles which may denature the compound and reduce potency.
- Keep detailed laboratory records including reconstitution dates, lot numbers, concentrations, and storage conditions.
- Dispose of unused material and sharps in accordance with local regulations and institutional biosafety guidelines.
Stability & Shelf Life
Lyophilized (freeze-dried) peptides are highly stable when stored correctly. At -20°C (-4°F), most peptides retain >95% purity for 24 months or longer. Once reconstituted, the clock starts—proteins in solution are inherently less stable than in dry form. Factors that accelerate degradation include temperature fluctuations, exposure to light, repeated freeze-thaw cycles, bacterial contamination, and oxidation.
Purity & Quality Considerations
Research-grade compounds should be accompanied by a Certificate of Analysis (COA) confirming purity, typically verified by High-Performance Liquid Chromatography (HPLC) and Mass Spectrometry (MS). Look for purity levels of ≥98% for research applications. Third-party testing adds an additional layer of quality assurance. Always verify the source and documentation before using any research compound.
Research Supplies & Resources
Essential supplies and educational resources for peptide research. Links go to Amazon.com.
Lab Supplies
Recommended Reading
Lab Equipment
As an Amazon Associate, peptides.fyi earns from qualifying purchases. Learn more.