Synopsis
Compound overview
- Research only
- In clinical trials
- Approved outside US
- FDA-approved
What it is
NAD+ (nicotinamide adenine dinucleotide) is a coenzyme found in every living cell, central to energy production. It is sold as a supplement and given by IV in some clinics; NAD-boosting compounds are being studied in clinical research.
What it does
Recognised and studied roles include:
- Essential for cells to produce energy
- Involved in DNA repair and cell signalling
- Studied for roles in ageing and metabolism
- Levels naturally decline with age
How it works
NAD+ shuttles energy-carrying electrons inside cells and is used up by repair and signalling enzymes such as the sirtuins. Interest in "boosting" NAD+ comes from its natural decline as people get older.
Safety notes
NAD+ and its precursors are still being studied, and long-term benefits in healthy people are not established. IV NAD+ can cause flushing, nausea and chest tightness during infusion. Supplement quality varies, and claims often run ahead of the evidence.
Where to buy NAD+
Pre-measured, dial-adjustable dosing — no reconstitution or measuring. The simplest research format to work with.
Standard lyophilized vial — reconstitute and measure doses yourself. The conventional research format.
Affiliate links — we may earn a commission at no extra cost to you.
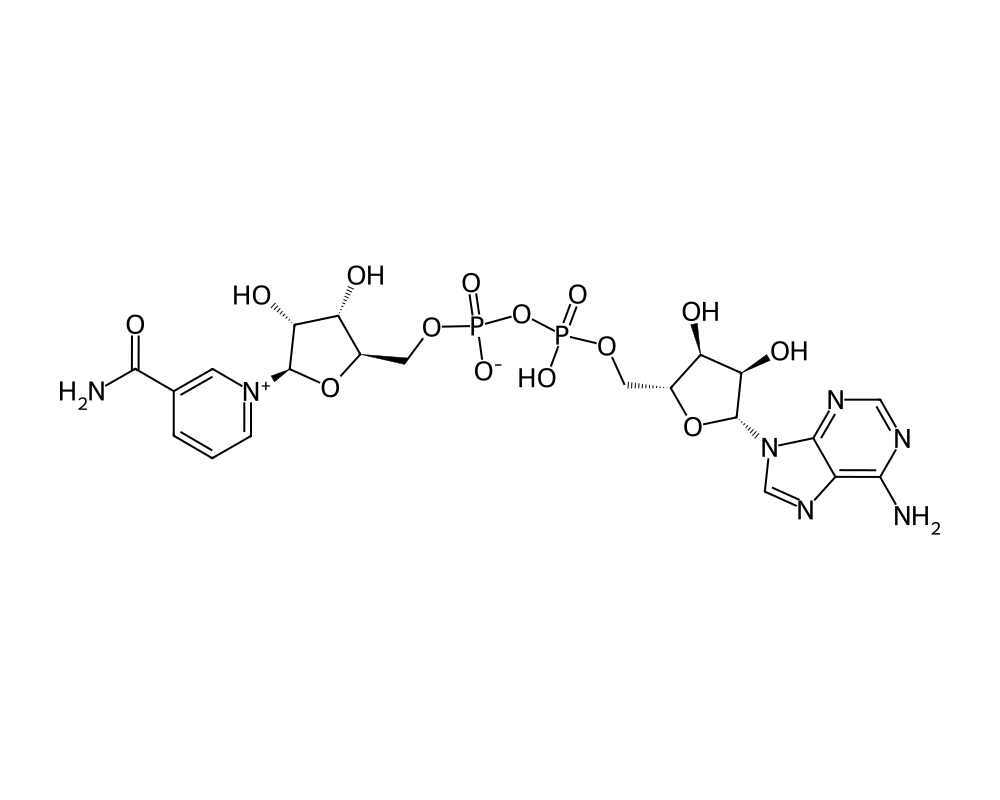
Molecular Structure
Research tool
Reconstitution calculator
Concentration
2.50mg/mL
Draw volume
0.10mL
Insulin units
10IU
Doses/vial
20
Overview
Nicotinamide adenine dinucleotide (NAD+) is not a peptide. It is a pyridine dinucleotide coenzyme present in every living cell, consisting of two nucleotides joined through their phosphate groups: one carrying an adenine base, the other carrying nicotinamide. The molecule is included here as a cofactor compound because it is sold by research peptide vendors alongside peptides and is the subject of a substantial research literature spanning aging biology, metabolism, and neurodegeneration.
Contents
NAD+ has two distinct biochemical roles. As a coenzyme in redox reactions, it cycles between its oxidized form (NAD+) and reduced form (NADH), accepting and donating electrons in glycolysis, the citric acid cycle, fatty acid oxidation, and oxidative phosphorylation. As a substrate, it is consumed by several enzyme families, sirtuins (NAD+-dependent deacylases), poly-ADP-ribose polymerases (PARPs, involved in DNA repair), and the ectoenzyme CD38, which cleave the molecule to perform post-translational protein modifications and signaling reactions.
Cellular NAD+ concentrations decline with age and in several metabolic disease states in multiple tissue types. This observation, advanced by laboratories led by David Sinclair (Harvard Medical School), Shin-ichiro Imai (Washington University), Eric Verdin (Buck Institute), and Charles Brenner (City of Hope), has motivated a research program around restoring NAD+ levels. The primary clinical strategy has been oral supplementation with NAD+ precursors, nicotinamide riboside (NR) and nicotinamide mononucleotide (NMN), which the cell converts to NAD+ through the salvage pathway. Direct injectable NAD+ research, sold by some research vendors, has a smaller published evidence base.
Mechanism of Action
Sirtuin Activation
The link between NAD+ and the aging-relevant sirtuin family was established by Imai et al. (2000, Nature), who demonstrated that the yeast Sir2 protein is an NAD+-dependent histone deacetylase. The seven mammalian sirtuins (SIRT1 through SIRT7) catalyze NAD+-consuming deacetylation, deacylation, and ADP-ribosylation reactions across nuclear, mitochondrial, and cytosolic compartments. Sirtuin activity is directly dependent on intracellular NAD+ availability, which has positioned NAD+ depletion as a candidate mechanism in age-related sirtuin decline.
PARP-Mediated DNA Repair
Poly-ADP-ribose polymerases (PARPs) consume NAD+ to attach poly-ADP-ribose chains to proteins at sites of DNA damage, recruiting repair machinery. PARP1, the most abundant family member, is a major sink for cellular NAD+, particularly under genotoxic stress. The competition between PARPs and sirtuins for a shared NAD+ pool is a central concept in the NAD+ aging literature.
CD38 Regulation
CD38 is a NAD+ glycohydrolase expressed on immune cells and other tissues. Its expression rises with age and chronic inflammation, providing a candidate mechanism for the observed age-related decline in tissue NAD+ levels. CD38 inhibitors are an active area of pharmacological research.
Mitochondrial Bioenergetics
Through its redox-cycling role, NAD+ availability constrains the flux of glycolysis and the citric acid cycle, both of which generate reducing equivalents (NADH) for the electron transport chain. Reduced cellular NAD+ has been associated with impaired mitochondrial function in several preclinical models.
Research Summary
NMN and Aging Biology
Yoshino et al. (2018, Cell Metabolism) reviewed the preclinical evidence for nicotinamide mononucleotide (NMN) as an NAD+ precursor, with rodent studies showing improvements in glucose tolerance, vascular function, and tissue NAD+ content. Mills et al. (2016, Cell Metabolism) reported that long-term NMN administration attenuated age-associated physiological decline in mice.
NR Oral Bioavailability
Trammell et al. (2016, Nature Communications) characterized nicotinamide riboside (NR) pharmacokinetics in humans, demonstrating dose-dependent increases in blood NAD+ following oral administration. NR is now sold as a dietary supplement under several brand names, with ongoing trials in metabolic and cardiovascular indications.
Neurodegeneration
Verdin (2015, Science) reviewed the evidence for NAD+ involvement in neurodegenerative disease, with particular focus on the SARM1 pathway and Wallerian axonal degeneration. NAD+ supplementation has been studied preclinically in Alzheimer’s, Parkinson’s, and amyotrophic lateral sclerosis models.
Direct Injectable NAD+
Research using injectable NAD+ rather than precursors is comparatively sparse in the peer-reviewed literature. Most published clinical and preclinical aging work has used NR or NMN, which carry better pharmacokinetic profiles for systemic delivery. The mechanism by which intravenously or subcutaneously administered NAD+ would reach intracellular pools has not been fully characterized; current evidence suggests breakdown to nicotinamide and subsequent salvage rather than direct uptake of intact NAD+.
Research Status
NAD+ is an endogenous coenzyme; deficiency states (pellagra, from severe niacin deficiency) are clinically established. As a research compound for aging or metabolic indications, the oral precursors NR and NMN have the deepest published record, with multiple Phase II human trials. Direct NAD+ administration as a research compound has a thinner peer-reviewed literature base, and pharmacokinetic interactions between injected NAD+ and the cellular salvage pathway remain incompletely characterized.
Further reading: NAD+ and Cellular Aging reviews the longevity research on NAD+ decline and cellular aging.
Dosing in Published Research
About this section
The information below reports dosing only as it appears in published clinical or preclinical research and official regulatory documents. It is provided as published-literature reference material. It is not dosing guidance, not medical advice, and not a recommendation to use or self-administer this compound.
NAD+ (nicotinamide adenine dinucleotide) is a coenzyme found in every cell. NAD+ itself is not well absorbed by mouth and has no established oral dose, and intravenous NAD+ infusions, although marketed commercially, are not supported by an established dose or by controlled efficacy trials. Most human research on raising NAD+ instead uses precursor molecules: clinical trials of nicotinamide riboside have used roughly 250 to 1,000 mg twice daily, and trials of nicotinamide mononucleotide have used roughly 150 to 1,200 mg per day. These figures describe precursor doses studied in specific trials, not doses of NAD+ itself.
Research doses, not a protocol
The figures above are for NAD+ precursor compounds studied in research settings; they are not an established dose for NAD+ itself, and intravenous NAD+ is not an FDA-approved therapy. Material sold for research use is not a regulated drug product.
Frequently Asked Questions
What is NAD+?
NAD+ (nicotinamide adenine dinucleotide) is a coenzyme found in every living cell and central to energy production. It is a pyridine dinucleotide rather than a peptide, and is included on this site as a cofactor entry.
How does NAD+ work?
NAD+ shuttles energy-carrying electrons through central metabolism and also serves as a substrate consumed by enzymes such as sirtuins, which are involved in DNA repair and cell signalling. Cellular NAD+ levels naturally decline with age.
Is NAD+ FDA-approved?
NAD+ itself is not an FDA-approved drug. Deficiency states such as pellagra are clinically established, but for aging or metabolic indications NAD+ and its precursors are still under clinical investigation.
What does the research say about NAD+?
The oral precursors NR and NMN have the deepest published record, with multiple Phase II human trials showing they can raise NAD+ levels, and rodent studies report metabolic improvements. Evidence that boosting NAD+ slows human aging remains preliminary.
What are the safety concerns with NAD+?
Oral NAD+ precursors have generally been reported as well tolerated in short trials. Direct intravenous NAD+ can cause infusion-related discomfort when given quickly, and long-term safety data for NAD+-boosting approaches is still limited.
Research Handling & Storage
Reconstitution (General Guidelines)
Lyophilized peptides are typically reconstituted using bacteriostatic water (0.9% benzyl alcohol). Standard reconstitution protocol:
- Remove the vial from storage and allow it to reach room temperature (20–25°C / 68–77°F) before opening. This typically takes 15–20 minutes.
- Clean the vial stopper with an alcohol prep pad and allow to air dry.
- Using a sterile syringe, slowly inject bacteriostatic water along the inside wall of the vial. Do not spray directly onto the lyophilized powder.
- Gently swirl the vial until the powder is fully dissolved. Do not shake vigorously as this may damage the peptide structure.
- The reconstituted solution should be clear and colorless. Discard if cloudy, discolored, or if particulate matter is visible.
- Label the vial with the reconstitution date, concentration, and your initials.
Common reconstitution volumes in research: 1ml or 2ml of bacteriostatic water per vial, depending on the desired concentration. For example, adding 2ml to a 5mg vial yields a concentration of 2.5mg/ml (2,500mcg/ml).
Storage
- Lyophilized (unreconstituted): Store at -20°C (-4°F) for long-term storage (stable 24+ months), or 2–8°C (36–46°F) refrigerated for short-term storage up to 6 months. Keep desiccated and protected from light.
- Reconstituted: Store at 2–8°C (36–46°F) refrigerated. Use within 4–6 weeks of reconstitution. Do not freeze reconstituted solutions as this may cause degradation.
- Shipping: Lyophilized peptides are generally stable at ambient temperature during transit for several days. Reconstituted solutions should be shipped on ice packs.
Handling Precautions
- Handle with appropriate personal protective equipment (PPE) including nitrile gloves, lab coat, and eye protection.
- Use aseptic/sterile technique when reconstituting and transferring solutions to prevent contamination.
- Avoid repeated freeze-thaw cycles which may denature the compound and reduce potency.
- Keep detailed laboratory records including reconstitution dates, lot numbers, concentrations, and storage conditions.
- Dispose of unused material and sharps in accordance with local regulations and institutional biosafety guidelines.
Stability & Shelf Life
Lyophilized (freeze-dried) peptides are highly stable when stored correctly. At -20°C (-4°F), most peptides retain >95% purity for 24 months or longer. Once reconstituted, the clock starts—proteins in solution are inherently less stable than in dry form. Factors that accelerate degradation include temperature fluctuations, exposure to light, repeated freeze-thaw cycles, bacterial contamination, and oxidation.
Purity & Quality Considerations
Research-grade compounds should be accompanied by a Certificate of Analysis (COA) confirming purity, typically verified by High-Performance Liquid Chromatography (HPLC) and Mass Spectrometry (MS). Look for purity levels of ≥98% for research applications. Third-party testing adds an additional layer of quality assurance. Always verify the source and documentation before using any research compound.
Research Supplies & Resources
Essential supplies and educational resources for peptide research. Links go to Amazon.com.
Lab Supplies
Recommended Reading
Lab Equipment
As an Amazon Associate, peptides.fyi earns from qualifying purchases. Learn more.