Synopsis
Compound overview
- Research only
- In clinical trials
- Approved outside US
- FDA-approved
What it is
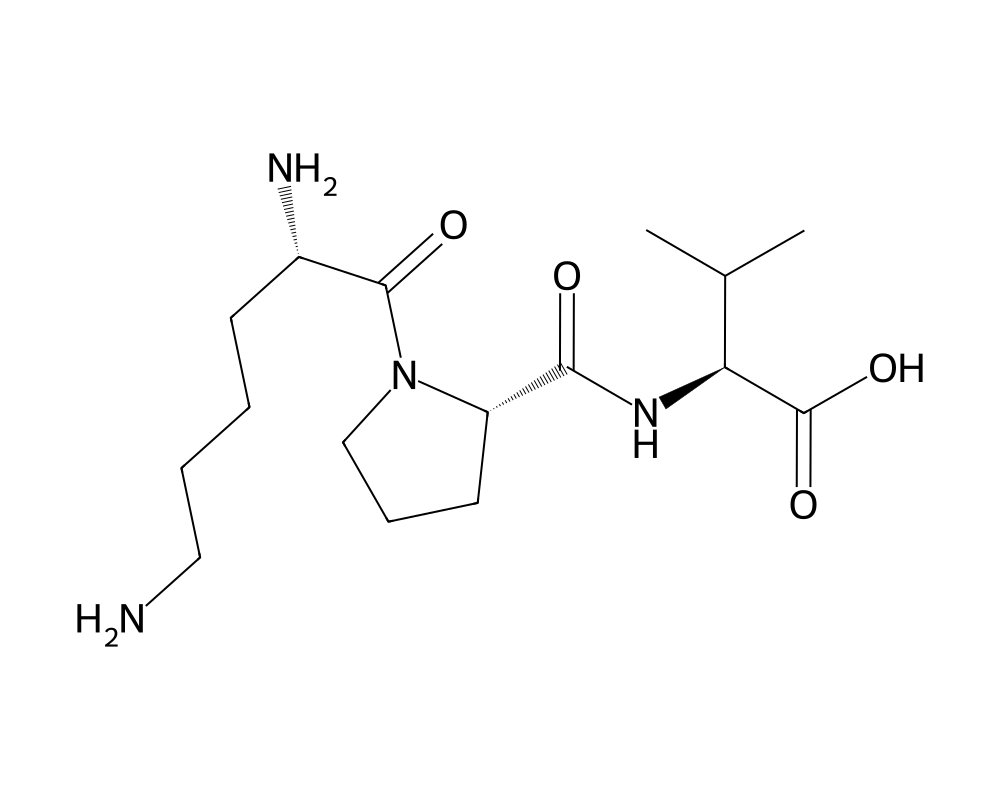
KPV is a tripeptide — just three amino acids (lysine, proline, valine) — that forms the tail end of the natural hormone alpha-MSH. It is sold only as a research chemical and is not an approved drug.
What it does
Areas explored in research include:
- Studied for anti-inflammatory effects in lab models
- Researched for gut and skin inflammation
- Investigated in wound-related research
- Small and stable compared with larger peptides
How it works
Research suggests KPV can enter cells and dampen inflammatory signalling, including a pathway called NF-kB, which helps explain the anti-inflammatory effects seen in laboratory studies.
Safety notes
KPV has no completed human trials and no approved-medicine safety record, so its human safety profile is unknown. Research-grade purity varies between suppliers. Any human use should be considered experimental.
Where to buy KPV
Standard lyophilized vial — reconstitute and measure doses yourself. The conventional research format.
Affiliate links — we may earn a commission at no extra cost to you.
Molecular Structure
Research tool
Reconstitution calculator
Concentration
2.50mg/mL
Draw volume
0.10mL
Insulin units
10IU
Doses/vial
20
Overview
KPV is a synthetic tripeptide composed of three amino acids (lysine-proline-valine) corresponding to residues 11-13 at the C-terminus of alpha-melanocyte-stimulating hormone (alpha-MSH). The parent peptide, alpha-MSH, is a 13-amino-acid hormone with a long-documented anti-inflammatory and immunomodulatory role. Work by James Lipton, Anna Catania, and collaborators at the University of Tennessee in the 1990s identified the C-terminal tripeptide as the smallest fragment retaining a substantial portion of alpha-MSH’s anti-inflammatory activity (Lipton and Catania, 1997, Immunology Today).
Contents
Unlike full-length alpha-MSH, which also engages melanocortin receptors involved in pigmentation, appetite, and steroidogenesis, KPV appears to act primarily through an anti-inflammatory route without strongly engaging the canonical melanocortin pigmentary functions. That dissociation, combined with the molecule’s small size and oral and intestinal stability, has made it a recurring focus of preclinical investigation for inflammatory conditions where alpha-MSH’s broader receptor activity would be confounding.
Mechanism of Action
The molecular pathways through which KPV exerts its anti-inflammatory effect are not fully resolved. Several mechanisms have been proposed and supported by experimental data.
NF-kB Pathway Suppression
Work by Brzoska and colleagues (2008, Endocrine Reviews) on the melanocortin anti-inflammatory cascade described suppression of the NF-kB transcription factor as a shared mechanism for both alpha-MSH and its C-terminal fragments. KPV reduced nuclear translocation of the p65 NF-kB subunit in cultured keratinocytes and intestinal epithelial cells.
Cytokine Modulation
Across multiple animal models, KPV administration has been associated with reductions in pro-inflammatory cytokines including TNF-alpha, IL-6, and IL-1beta. Dalmasso et al. (2008, Gastroenterology) reported that nanoparticle-encapsulated KPV reduced colonic levels of these cytokines in a dextran sulfate sodium (DSS) mouse model of colitis at doses several orders of magnitude lower than free peptide.
Mast Cell Stabilization
Independent studies have reported attenuation of mast cell degranulation in skin models. The receptor mediating this effect remains a matter of investigation, with some evidence suggesting an intracellular site of action accessed through PEPT1-mediated peptide transport in intestinal epithelial cells.
Research Summary
Inflammatory Bowel Disease Models
The most extensive preclinical record for KPV is in models of inflammatory bowel disease. Kannengiesser et al. (2008, Inflammatory Bowel Diseases) demonstrated attenuation of colitis in mice receiving oral KPV. The Dalmasso 2008 study showed that nanoparticle delivery further reduced the effective dose by targeting the peptide to colonic epithelial cells, reducing histologic damage scores and cytokine output.
Atopic Dermatitis and Skin Inflammation
Brzoska, Luger, and colleagues at the University of Muenster have published a series of reports characterizing alpha-MSH and KPV in models of dermatitis. The 2008 Endocrine Reviews article summarized the case for melanocortin-derived peptides in inflammatory skin disease and noted KPV as a candidate with reduced pigmentary side effects compared to alpha-MSH.
Mucosal Wound Healing
Smaller preclinical studies have reported effects on corneal and intestinal mucosal healing, though the literature is less extensive than the colitis work.
Research Status
KPV remains a research compound. No KPV product is approved by the FDA, EMA, or any major regulatory agency for human therapeutic use. Published clinical trial data in humans is essentially absent, with most work to date conducted in cultured cells and rodent disease models. The combination of small molecular size, apparent oral activity, and dissociation from melanocortin pigmentation effects has sustained academic interest, but the regulatory and clinical record remains limited.
Further reading: KPV is one of the four peptides in the KLOW peptide blend, studied with GHK-Cu, BPC-157, and TB-500.
Dosing in Published Research
About this section
The information below reports dosing only as it appears in published clinical or preclinical research and official regulatory documents. It is provided as published-literature reference material. It is not dosing guidance, not medical advice, and not a recommendation to use or self-administer this compound.
KPV is a short tripeptide fragment related to alpha-melanocyte-stimulating hormone. Research on KPV has been conducted in laboratory and animal models of inflammation; no controlled human clinical trial has established a dose for it. Specific figures circulating in forums or vendor material are not derived from human research and are therefore not reported here.
No established human dosing
Because no human trial has established a dose for KPV, any specific figures circulating online are unverified. KPV is not an approved drug product, and material sold under this name is for laboratory research use only.
Frequently Asked Questions
What is KPV?
KPV is a synthetic tripeptide made of three amino acids (lysine-proline-valine) corresponding to the C-terminal tail (residues 11 to 13) of the hormone alpha-melanocyte-stimulating hormone (alpha-MSH). It is sold only as a research chemical and is not an approved drug.
How does KPV work?
The molecular pathways are not fully resolved. Experimental work suggests KPV can enter cells and dampen inflammatory signalling, with proposed mechanisms including suppression of the NF-kB pathway downstream of the melanocortin anti-inflammatory system.
Is KPV FDA-approved?
No. No KPV product is approved by the FDA, the EMA or any major regulatory agency for human therapeutic use. It remains a research compound.
What does the research say about KPV?
The most extensive preclinical record is in inflammatory bowel disease models, where studies have reported reduced colitis in mice given KPV. The work to date is concentrated in cultured cells and rodent disease models.
Are there human studies of KPV?
Published clinical trial data in humans is essentially absent. The available evidence comes from laboratory and animal research, so firm conclusions about effects or safety in people cannot yet be drawn.
Research Handling & Storage
Reconstitution (General Guidelines)
Lyophilized peptides are typically reconstituted using bacteriostatic water (0.9% benzyl alcohol). Standard reconstitution protocol:
- Remove the vial from storage and allow it to reach room temperature (20–25°C / 68–77°F) before opening. This typically takes 15–20 minutes.
- Clean the vial stopper with an alcohol prep pad and allow to air dry.
- Using a sterile syringe, slowly inject bacteriostatic water along the inside wall of the vial. Do not spray directly onto the lyophilized powder.
- Gently swirl the vial until the powder is fully dissolved. Do not shake vigorously as this may damage the peptide structure.
- The reconstituted solution should be clear and colorless. Discard if cloudy, discolored, or if particulate matter is visible.
- Label the vial with the reconstitution date, concentration, and your initials.
Common reconstitution volumes in research: 1ml or 2ml of bacteriostatic water per vial, depending on the desired concentration. For example, adding 2ml to a 5mg vial yields a concentration of 2.5mg/ml (2,500mcg/ml).
Storage
- Lyophilized (unreconstituted): Store at -20°C (-4°F) for long-term storage (stable 24+ months), or 2–8°C (36–46°F) refrigerated for short-term storage up to 6 months. Keep desiccated and protected from light.
- Reconstituted: Store at 2–8°C (36–46°F) refrigerated. Use within 4–6 weeks of reconstitution. Do not freeze reconstituted solutions as this may cause degradation.
- Shipping: Lyophilized peptides are generally stable at ambient temperature during transit for several days. Reconstituted solutions should be shipped on ice packs.
Handling Precautions
- Handle with appropriate personal protective equipment (PPE) including nitrile gloves, lab coat, and eye protection.
- Use aseptic/sterile technique when reconstituting and transferring solutions to prevent contamination.
- Avoid repeated freeze-thaw cycles which may denature the compound and reduce potency.
- Keep detailed laboratory records including reconstitution dates, lot numbers, concentrations, and storage conditions.
- Dispose of unused material and sharps in accordance with local regulations and institutional biosafety guidelines.
Stability & Shelf Life
Lyophilized (freeze-dried) peptides are highly stable when stored correctly. At -20°C (-4°F), most peptides retain >95% purity for 24 months or longer. Once reconstituted, the clock starts—proteins in solution are inherently less stable than in dry form. Factors that accelerate degradation include temperature fluctuations, exposure to light, repeated freeze-thaw cycles, bacterial contamination, and oxidation.
Purity & Quality Considerations
Research-grade compounds should be accompanied by a Certificate of Analysis (COA) confirming purity, typically verified by High-Performance Liquid Chromatography (HPLC) and Mass Spectrometry (MS). Look for purity levels of ≥98% for research applications. Third-party testing adds an additional layer of quality assurance. Always verify the source and documentation before using any research compound.
Research Supplies & Resources
Essential supplies and educational resources for peptide research. Links go to Amazon.com.
Lab Supplies
Recommended Reading
Lab Equipment
As an Amazon Associate, peptides.fyi earns from qualifying purchases. Learn more.