Synopsis
Compound overview
- Research only
- In clinical trials
- Approved outside US
- FDA-approved
What it is
PT-141 (bremelanotide) is a synthetic peptide related to the melanocortin system. It is FDA-approved and sold by prescription as Vyleesi, used to treat low sexual desire in some pre-menopausal women.
What it does
Documented and studied effects include:
- Approved to treat hypoactive sexual desire disorder in women
- Studied for sexual arousal in both sexes
- Acts on the nervous system rather than blood flow
- Has documented clinical-trial data
How it works
Unlike erectile-dysfunction drugs that work on blood vessels, PT-141 activates melanocortin receptors in the brain that are involved in sexual desire and arousal.
Safety notes
PT-141 is prescription-only. Reported side effects include nausea, flushing, headache and temporary increases in blood pressure, so it is not suitable for people with uncontrolled high blood pressure or heart disease. Research-vendor material is not pharmacy-grade and is sold outside its approved use.
Where to buy PT-141 (Bremelanotide)
Standard lyophilized vial — reconstitute and measure doses yourself. The conventional research format.
Affiliate links — we may earn a commission at no extra cost to you.
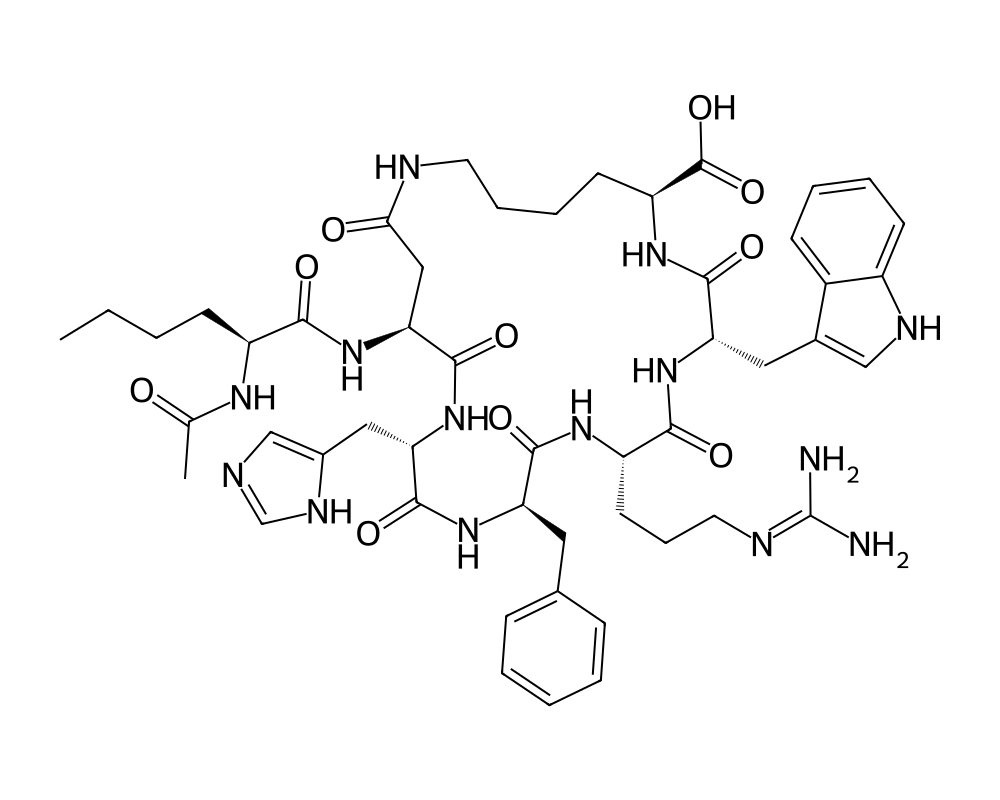
Molecular Structure
Research tool
Reconstitution calculator
Concentration
2.50mg/mL
Draw volume
0.10mL
Insulin units
10IU
Doses/vial
20
Overview
PT-141, known by its generic name bremelanotide, is a cyclic heptapeptide melanocortin receptor agonist that was derived from the research peptide Melanotan II (MT-II). It was developed by Palatin Technologies and received FDA approval in June 2019 under the brand name Vyleesi for the treatment of acquired, generalized hypoactive sexual desire disorder (HSDD) in premenopausal women, making it the first melanocortin-based therapeutic to achieve regulatory approval.
Contents
- Overview
- Mechanism of Action
- MC4R Activation in the Hypothalamus
- MC3R Modulation
- Distinction from Peripheral Mechanisms
- Research Summary
- Early Erectile Dysfunction Studies
- Female Sexual Dysfunction Research
- RECONNECT Phase III Trials
- Safety and Tolerability
- Dosing in Published Research
- Safety and Side Effects
- Current Research Status
- Frequently Asked Questions
The discovery of PT-141’s effects on sexual function was serendipitous. During early clinical trials of Melanotan II as a tanning agent in the 1990s at the University of Arizona, male subjects reported spontaneous penile erections as an unexpected side effect. This observation prompted systematic investigation of the melanocortin system’s role in sexual arousal, leading to the identification of the MC3R and MC4R receptor subtypes as mediators of central sexual response.
Structurally, PT-141 is the active carboxylic acid metabolite of Melanotan II, differing by the absence of the N-terminal acetyl and C-terminal amide groups. Despite this structural similarity, PT-141 was specifically optimized for its central nervous system effects on sexual function rather than melanogenesis, and it represents a fundamentally novel mechanism for addressing sexual dysfunction by acting through the central melanocortin system rather than through peripheral vascular mechanisms employed by phosphodiesterase type 5 (PDE5) inhibitors.
Mechanism of Action
PT-141 acts through a centrally mediated mechanism that distinguishes it from all previously approved treatments for sexual dysfunction. Its pharmacological target is the melanocortin receptor system in the hypothalamus and limbic structures.
MC4R Activation in the Hypothalamus
The primary mechanism of PT-141 involves agonism of melanocortin-4 receptors (MC4R) in the medial preoptic area (MPOA) and paraventricular nucleus (PVN) of the hypothalamus. Activation of MC4R in these regions stimulates oxytocinergic neurons that project to the spinal cord via descending pathways. Oxytocin release at the level of the sacral parasympathetic nucleus (S2-S4) activates autonomic outflow to genital tissues, facilitating both physiological arousal responses (genital vasocongestion, lubrication) and the subjective experience of sexual desire through concurrent activation of limbic reward circuits.
MC3R Modulation
PT-141 also activates MC3R, which is expressed in the ventromedial hypothalamus and arcuate nucleus. While MC4R is considered the primary mediator of the sexual response, MC3R activation appears to contribute to the motivational and appetitive components of sexual behavior. Preclinical studies by Pfaus et al. demonstrated that MC3R signaling modulates dopaminergic neurotransmission in the mesolimbic reward pathway, potentially enhancing the incentive salience of sexual stimuli and contributing to the subjective experience of desire.
Distinction from Peripheral Mechanisms
Unlike PDE5 inhibitors (sildenafil, tadalafil) that act exclusively on peripheral vascular smooth muscle to enhance blood flow, PT-141 initiates the sexual response cascade at its neural origin. This central mechanism means PT-141 can influence both the desire/motivational component and the physiological arousal component of sexual response. The downstream signaling involves activation of endothelial nitric oxide synthase (eNOS) in genital vasculature, but this occurs as a consequence of central neural activation rather than direct pharmacological vasodilation.
Research Summary
The clinical development of PT-141 spans nearly two decades, with research initially focused on erectile dysfunction before pivoting to HSDD in women based on emerging clinical data.
Early Erectile Dysfunction Studies
Diamond et al. (2004), published in the International Journal of Impotence Research, conducted a double-blind, placebo-controlled study of intranasal PT-141 in 20 men with erectile dysfunction. The study demonstrated that PT-141 produced clinically significant erections as measured by RigiScan monitoring, with a dose-dependent response. Notably, PT-141 was effective in patients who had previously failed to respond to sildenafil, suggesting its central mechanism could bypass peripheral vascular limitations.
Female Sexual Dysfunction Research
Pfaus et al. (2007), published in Hormones and Behavior, provided comprehensive preclinical evidence that melanocortin agonists facilitated female sexual behavior in rodent models through central mechanisms involving the MPOA and ventromedial hypothalamus. These findings provided the scientific rationale for clinical investigation of PT-141 in female sexual dysfunction.
RECONNECT Phase III Trials
Kingsberg et al. (2019), published in Obstetrics & Gynecology, reported results from the two pivotal RECONNECT Phase III trials that supported FDA approval. Across both studies enrolling over 1,200 premenopausal women with HSDD, subcutaneous bremelanotide 1.75 mg administered on an as-needed basis significantly increased the number of satisfying sexual events (SSE) and improved scores on the Female Sexual Distress Scale-Desire/Arousal/Orgasm (FSDS-DAO) compared to placebo. The mean increase in SSE was approximately 1.0 event per month, with 35-38% of participants achieving a clinically meaningful response versus 28-31% with placebo.
Safety and Tolerability
Clayton et al. (2016), published in the Journal of Sexual Medicine, reported the long-term safety profile of bremelanotide from open-label extension studies. The most common adverse effect was nausea (approximately 40% of patients), which was typically mild, transient, and diminished with repeated dosing. Transient increases in blood pressure of 2-3 mmHg were observed within 12 hours of administration, leading to a contraindication in patients with uncontrolled hypertension. Importantly, no significant melanogenic effects were observed at the therapeutic dose, distinguishing it pharmacologically from its parent compound Melanotan II.
Dosing in Published Research
About this section
The information below reports dosing only as it appears in published clinical or preclinical research and official regulatory documents. It is provided as published-literature reference material. It is not dosing guidance, not medical advice, and not a recommendation to use or self-administer this compound.
PT-141 is also known as bremelanotide and is an FDA-approved prescription medicine, sold as Vyleesi. According to the FDA-approved labeling, the dose is 1.75 mg injected subcutaneously into the abdomen or thigh, on an as-needed basis, at least 45 minutes before anticipated sexual activity, for premenopausal women with acquired, generalized hypoactive sexual desire disorder. Labeling limits use to one dose in any 24-hour period and no more than eight doses per month. These figures are drawn from FDA-approved prescribing information.
Important
The dose above applies to the approved prescription product, studied in a specific patient population under medical supervision. It is not a recommendation, and it does not apply to material sold for laboratory or research use, which is not the approved drug product. Bremelanotide can transiently raise blood pressure and is not labeled for use in people with uncontrolled hypertension or known cardiovascular disease.
Safety and Side Effects
PT-141 (bremelanotide) is an FDA-approved drug, and its safety profile is reasonably well characterized. The most common adverse effects are nausea, which can be pronounced and is most likely with the first dose, along with flushing, headache, and injection-site reactions. Clinically important is its effect on the cardiovascular system: bremelanotide causes transient increases in blood pressure and reductions in heart rate after each dose, so it is contraindicated in people with uncontrolled hypertension or known cardiovascular disease, and it should not be used by those at high cardiovascular risk. Use is limited to no more than one dose in any 24-hour period and no more than eight doses per month. Focal hyperpigmentation, including darkening of the face, gums, and breasts, has been reported, more often with frequent dosing or in people with darker skin, and may not fully resolve. Nausea and related effects led a meaningful minority of trial participants to discontinue treatment.
Current Research Status
Bremelanotide is an FDA-approved prescription medication, marketed as Vyleesi, approved in 2019 for acquired, generalized hypoactive sexual desire disorder in premenopausal women. Its approval is specific to that population and indication; use outside it, including in men or for general sexual enhancement, is off-label and not supported by the approval. As a prescription drug it should be used under medical supervision, and material sold outside the regulated pharmacy supply chain is of uncertain identity, dose, and purity.
Frequently Asked Questions
What is PT-141 (Bremelanotide)?
PT-141, generic name bremelanotide, is a synthetic cyclic heptapeptide that acts on the melanocortin system, derived from the earlier research peptide Melanotan II. It is FDA-approved and sold by prescription as Vyleesi.
How does PT-141 work?
Unlike erectile-dysfunction drugs that work on blood flow, PT-141 acts centrally, on melanocortin receptors (chiefly MC4R) in the hypothalamus and related brain structures. This central mechanism is what distinguishes it from previously approved sexual-dysfunction treatments.
Is PT-141 FDA-approved?
Yes, for one specific use. Bremelanotide was approved by the FDA in 2019 as Vyleesi for acquired, generalized hypoactive sexual desire disorder in premenopausal women. Use outside that population, including in men, is off-label.
What does the research say about PT-141?
PT-141’s clinical development spans nearly two decades, initially in erectile dysfunction before pivoting to hypoactive sexual desire disorder in women, where trial data supported its approval as Vyleesi.
What are the safety concerns with PT-141?
As an FDA-approved drug its safety profile is reasonably well characterized. The most common adverse effects are nausea, which can be pronounced and is most likely with the first dose, along with flushing, headache and injection-site reactions. It can also transiently raise blood pressure.
Research Handling & Storage
Reconstitution (General Guidelines)
Lyophilized peptides are typically reconstituted using bacteriostatic water (0.9% benzyl alcohol). Standard reconstitution protocol:
- Remove the vial from storage and allow it to reach room temperature (20–25°C / 68–77°F) before opening. This typically takes 15–20 minutes.
- Clean the vial stopper with an alcohol prep pad and allow to air dry.
- Using a sterile syringe, slowly inject bacteriostatic water along the inside wall of the vial. Do not spray directly onto the lyophilized powder.
- Gently swirl the vial until the powder is fully dissolved. Do not shake vigorously as this may damage the peptide structure.
- The reconstituted solution should be clear and colorless. Discard if cloudy, discolored, or if particulate matter is visible.
- Label the vial with the reconstitution date, concentration, and your initials.
Common reconstitution volumes in research: 1ml or 2ml of bacteriostatic water per vial, depending on the desired concentration. For example, adding 2ml to a 5mg vial yields a concentration of 2.5mg/ml (2,500mcg/ml).
Storage
- Lyophilized (unreconstituted): Store at -20°C (-4°F) for long-term storage (stable 24+ months), or 2–8°C (36–46°F) refrigerated for short-term storage up to 6 months. Keep desiccated and protected from light.
- Reconstituted: Store at 2–8°C (36–46°F) refrigerated. Use within 4–6 weeks of reconstitution. Do not freeze reconstituted solutions as this may cause degradation.
- Shipping: Lyophilized peptides are generally stable at ambient temperature during transit for several days. Reconstituted solutions should be shipped on ice packs.
Handling Precautions
- Handle with appropriate personal protective equipment (PPE) including nitrile gloves, lab coat, and eye protection.
- Use aseptic/sterile technique when reconstituting and transferring solutions to prevent contamination.
- Avoid repeated freeze-thaw cycles which may denature the compound and reduce potency.
- Keep detailed laboratory records including reconstitution dates, lot numbers, concentrations, and storage conditions.
- Dispose of unused material and sharps in accordance with local regulations and institutional biosafety guidelines.
Stability & Shelf Life
Lyophilized (freeze-dried) peptides are highly stable when stored correctly. At -20°C (-4°F), most peptides retain >95% purity for 24 months or longer. Once reconstituted, the clock starts—proteins in solution are inherently less stable than in dry form. Factors that accelerate degradation include temperature fluctuations, exposure to light, repeated freeze-thaw cycles, bacterial contamination, and oxidation.
Purity & Quality Considerations
Research-grade compounds should be accompanied by a Certificate of Analysis (COA) confirming purity, typically verified by High-Performance Liquid Chromatography (HPLC) and Mass Spectrometry (MS). Look for purity levels of ≥98% for research applications. Third-party testing adds an additional layer of quality assurance. Always verify the source and documentation before using any research compound.
Research Supplies & Resources
Essential supplies and educational resources for peptide research. Links go to Amazon.com.
Lab Supplies
Recommended Reading
Lab Equipment
As an Amazon Associate, peptides.fyi earns from qualifying purchases. Learn more.